
Focus on Heart Failure | A Long Road With Many Opportunities For Prevention

Despite breakthroughs in pharmacologic therapy, device-based treatment, and advanced circulatory and surgical support that have revolutionized heart failure (HF) management, the prevalence of HF continues to rise.1 Globally, there has been more than a doubling between 1990 and 2021 in the number of individuals living with HF.2 In the U.S., over 6.7 million adults live with HF, a number expected to surpass 8.7 million by 2030.3
These trends reveal a breaking reality: the traditional symptom-based approach is insufficient. Preventing HF earlier in the cardiovascular lifespan is now essential.
Prevention was placed at the forefront of HF care in a Joint Scientific Statement released in August 2025 by the Failure Society of America and the American Society for Preventive Cardiology.4 In The Continuum of Prevention and Heart Failure in Cardiovascular Medicine, HF prevention was defined not as a separate goal but as an essential component of longitudinal cardiovascular care.
This framework highlights that HF begins years before symptoms emerge, through the silent accumulation of structural, biochemical and hemodynamic changes. This prevention perspective is increasingly recognized globally and was reinforced by a three-part Heart Failure Prevention Series published the same month in The Lancet, which collectively demonstrate that HF evolves over decades.5-7
Before Symptoms Start: The Critical Window of Pre-Clinical HF
HF is best understood along a four-stage continuum, A through D, that reflects progressive changes in risk, structure and clinical presentation.8 Stage A includes individuals with common cardiometabolic and renal conditions that elevate HF risk despite normal cardiac structure and no symptoms. In practice, this stage should trigger routine HF risk assessment and aggressive risk-factor treatment such as blood pressure control, early metabolic therapies (SGLT2 inhibitors, GLP-1/GIP agents), weight-loss strategies and lipid optimization.4
Stage B ("pre-HF") identifies asymptomatic patients who already show early cardiac involvement, typically mild structural changes or elevated cardiac biomarkers.9 These findings indicate that myocardial stress has begun, and clinicians should escalate therapy rather than wait for symptoms. Evidence supports early use of guideline-directed medical therapy, metabolic optimization and evaluation for subclinical ischemia or valvular disease when appropriate.
For clinicians, Stages A and B should be approached as active phases of HF treatment, not passive descriptors. Embedding this prevention-first mindset by treating HF before it becomes apparent is the most effective way to change its lifelong trajectory.
Changing Face of Heart Failure
The profile of patients with HF has shifted dramatically over the last 35 years, with most now likely battling obesity, diabetes and kidney disease. This transformation, documented in a new study published in JACC, reveals both progress and a warning. While cardiology advances have reduced traditional risk factors, new metabolic issues have emerged. This reshaping of HF has important implications for patient care today and the design of clinical trials that will shape care tomorrow. Read more about these HF trends in the U.S.
A Cardiovascular-Kidney-Metabolic Framework For HF Prevention
Emerging work highlights that HF is the clinical expression of deeply interconnected cardiovascular, kidney and metabolic (CKM) dysfunction.10 CKM diseases frequently coexist, accumulate across the lifespan, and follow interrelated and often sequential pathobiology, creating a shared substrate for HF development. Contemporary epidemiological and therapeutic evidence demonstrates that CKM conditions are major, underrecognized drivers of HF onset, with risk magnitudes that often exceed that of traditional cardiac factors alone.7
CKM biology helps explain why HF develops even when traditional cardiac parameters look normal. Long before changes in LVEF, chamber size or natriuretic peptides are detectable, CKM conditions such as excess adiposity, dysglycemia, insulin resistance, hypertension, albuminuria and microvascular dysfunction generate energetic stress, inflammatory signaling and diastolic stiffening that quietly remodel the myocardium.11
This CKM lens reframes HF prevention as a multisystem intervention opportunity. Pharmacotherapies that exert parallel CKM benefits, including SGLT2 inhibitors, GLP-1 receptor agonists and GIP/GLP-1 co-agonists, underscore the shared biology linking these organ systems and highlight unprecedented opportunities for upstream HF prevention.7
For example, a 52-year-old woman with clinical obesity, prediabetes, microalbuminuria and mild hypertension with a normal LVEF and no symptoms. Historically, the risk of HF had not been considered as significant in this setting, however, within a CKM framework, her metabolic dysfunction and renal injury signal high susceptibility to HF with preserved ejection fraction (HFpEF), prompting early deployment of weight-modifying therapies, SGLT2 inhibition, blood pressure optimization and lifestyle strategies, even before any cardiac abnormalities appear.
Expanding the HF Prevention Lens
Additional to the CKM framework, a range of nontraditional factors also meaningfully shape HF trajectories and broaden the scope of prevention. Genetic predisposition plays a role for a small subset of individuals, with rare pathogenic variants associated with cardiomyopathy present in a minority of the general population.12 Also, sex-specific determinants are increasingly recognized as major drivers of HF risk.13
Women experience a disproportionate burden of HFpEF and demonstrate higher vulnerability to the adverse cardiovascular effects of diabetes, obesity and hypertension.14,15 Pregnancy-related complications, such as preeclampsia, gestational hypertension and diabetes, pregnancy loss, and peripartum cardiomyopathy, serve as powerful markers of future HF and cardiometabolic disease.15 Despite their strong predictive value, these reproductive and obstetric histories are often overlooked in routine cardiovascular assessments, representing a missed opportunity for early prevention.
Other nontraditional contributors include cancer therapies (anthracyclines, HER2-targeted agents, radiation), chronic psychosocial stress, depression, sleep disorders, and social and structural determinants such as limited access to nutritious foods, transportation barriers, financial hardship and environmental exposures.4
Collectively, these factors expand the preventive lens, emphasizing the need for a more comprehensive and individualized approach to HF risk assessment.
From Framework to Clinical Practice: Challenges and Opportunities
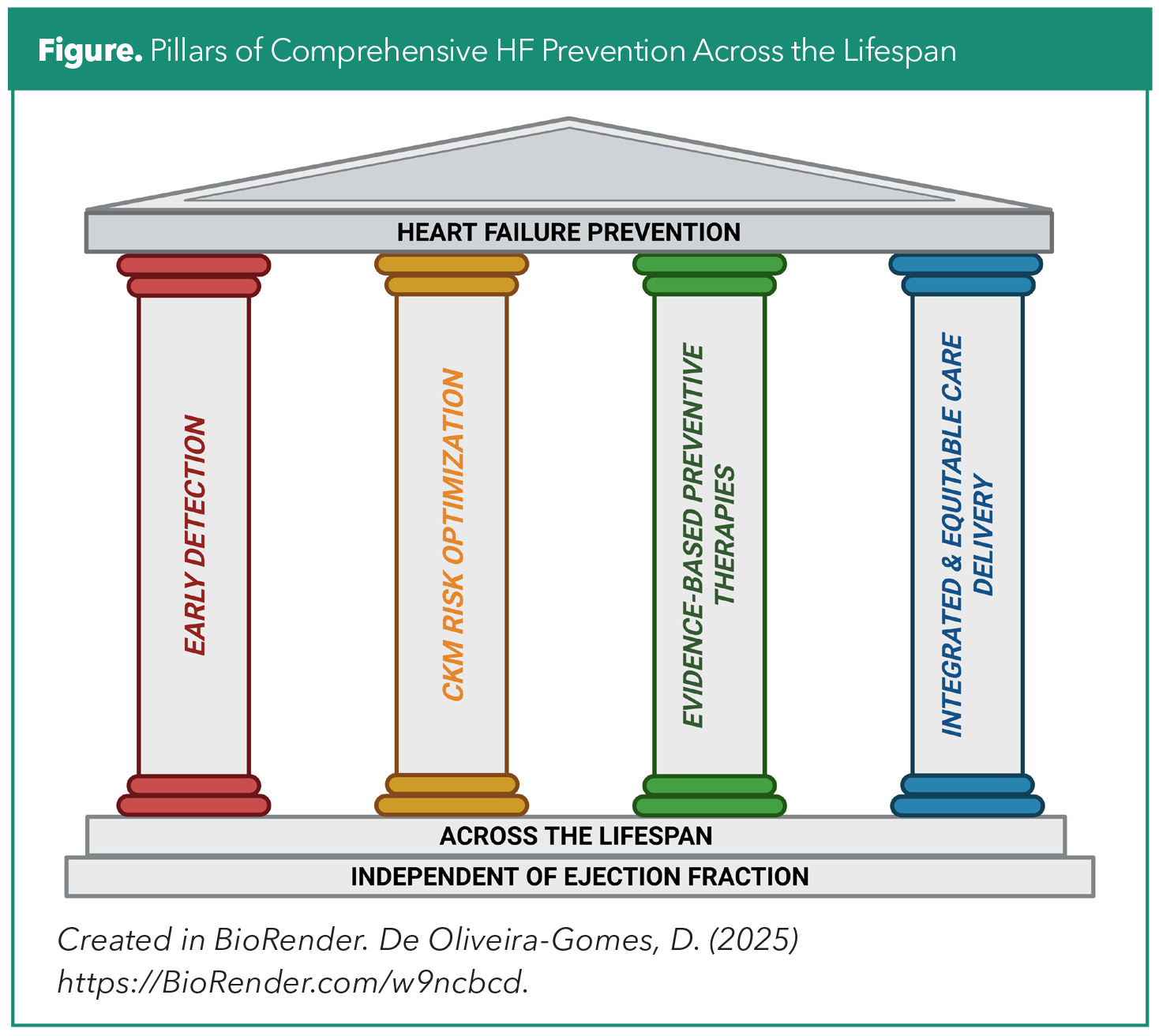
Translating a prevention-first HF vision into practice requires coordinated action across all levels of care (Figure). Clinically, prevention is strengthened by systematically identifying at-risk individuals using validated HF risk scores and integrating routine risk stratification into standard encounters. When risk is elevated, or when clinical suspicion persists, targeted use of biomarkers (natriuretic peptides, high-sensitivity troponin) and focused cardiac imaging can uncover early myocardial stress or subclinical dysfunction. Applying evidence-based therapies at this stage, before structural disease becomes established, enables intervention when it is most likely to modify trajectory and prevent progression.
Health systems have a critical role in operationalizing HF prevention. Integrated care pathways, multidisciplinary clinics, standardized HF risk tools within the electronic health record and expanded access to cardiac rehabilitation can help ensure that prevention strategies are consistently implemented. These models also bridge existing gaps between multiple specialties that should play an active role to prevent HF: preventive cardiology, primary care, nephrology, endocrinology and HF specialty practice.
At a population level, sustained progress in HF prevention depends on equitable access to preventive therapies and supportive services. Limitations in insurance coverage, medication affordability, transportation and community resources can hinder risk reduction efforts, particularly in populations disproportionately affected by cardiovascular disease. Addressing these social and structural barriers is essential to ensure that HF-prevention strategies translate into measurable improvements in public health.
In summary, a growing body of contemporary work converges on a clear conclusion: HF should no longer be viewed solely as an advanced clinical syndrome requiring complex therapy, but as a preventable condition shaped by cardiometabolic, renal and structural factors that accumulate across decades. Effective prevention depends on recognizing vulnerability early, treating risk factors aggressively and implementing therapies before irreversible myocardial injury develops. Adopting a prevention-first mindset and treating HF risk long before HF itself offers the strongest path to changing the future burden of the disease.
This article was authored by Diana De Oliveira Gomes, MD, Brigham and Women's Hospital, Harvard Medical School, Boston, MA; Christian Guilliod, MD, University of Miami/Jackson Health System, Miami, FL; and Vanessa Blumer, MD, FACC, Inova Schar Heart and Vascular Institute, Falls Church, VA.
References
- Martin SS, Aday AW, Allen NB, et al. 2025 heart disease and stroke statistics: a report of US and Global data from the American Heart Association. Circulation. 2025;151:e41-e660.
- Fonarow GC, Ahmad FS, Ahmad T, et al. HF STATS 2025: heart failure epidemiology and outcomes statistics an updated 2025 report from the Heart Failure Society of America. J Cardiac Fail. 2025;S1071-9164(25)00326-4.
- Bozkurt B, Ahmad T, Alexander KM, et al. Heart failure epidemiology and outcomes statistics: a report of the Heart Failure Society of America. J Card Fail. 2023;29:1412-51.
- Lala A, Beavers C, Blumer V, et al. The continuum of prevention and heart failure in cardiovascular medicine: a joint scientific statement from the Heart Failure Society of America and the American Society for Preventive Cardiology. J Cardiac Fail. 2025; S1071-9164(25)00327-6.
- Khan SS, Berwanger O, Fiuzat M, et al. Prioritising the primary prevention of heart failure. The Lancet. 2025;406:1138-53.
- Udell JA, Bahit MC, Campbell P, et al. Prevention of heart failure after acute myocardial infarction. The Lancet. 2025;406:1154-70.
- Ostrominski JW, Cheng AYY, Nelson AJ, et al. Cardiovascular, kidney, and metabolic health: an actionable vision for heart failure prevention. The Lancet. 2025;406:1171-92.
- Heidenreich PA, Bozkurt B, Aguilar D, et al. 2022 AHA/ACC/HFSA guideline for the Management of Heart Failure. JACC. 2022;79:e263-e421.
- Sebastian SA, Padda I, Johal G. Cardiovascular-kidney-metabolic (CKM) syndrome: A state-of-the-art review. Curr Probl Cardiol. 2024;49:102344.
- Ndumele CE, Neeland IJ, Tuttle KR, et al. A synopsis of the evidence for the science and clinical management of cardiovascular-kidney-metabolic (ckm) syndrome: a Scientific Statement From the American Heart Association. Circulation. 2023;148:1636-64.
- Bourfiss M, van Vugt M, Alasiri AI, et al. Prevalence and disease expression of pathogenic and likely pathogenic variants associated with inherited cardiomyopathies in the general population. Circ Genom Precis Med. 2022;15:e003704.
- Khan Sadiya S, Beach Lauren B, Yancy CW. Sex-based differences in heart failure. JACC. 2022;79:1530-41.
- Campbell P, Rutten FH, Lee MM, et al. Heart failure with preserved ejection fraction: everything the clinician needs to know. The Lancet. 2024;403:1083-92.
- Lala A, Tayal U, Hamo CE, et al. Sex differences in heart failure. J Card Fail. 2022;28:477-98.
Clinical Topics: Heart Failure and Cardiomyopathies, Prevention, Acute Heart Failure
Keywords: Cardiology Magazine, ACC Publications, CM-Jan-Feb-2026, Blood Pressure, Heart Failure, Primary Prevention, Sodium-Glucose Transporter 2 Inhibitors, Glucagon-Like Peptide 1, Risk Assessment