
Mental Stress-Induced Myocardial Ischemia: An Under-Recognized Cardiac Risk Factor?
Editor’s Note: Based on Jiang W, Samad Z, Boyle S, et al. Prevalence and Clinical Characteristics of Mental Stress–Induced Myocardial Ischemia in Patients With Coronary Heart Disease. J Am Coll Cardiol 2013;61:714-722.
Background
Mental stress induced myocardial ischemia (MSIMI) is common, with reported rates of up to 70% in patients with stable coronary heart disease (CHD) and associated with increased rates of subsequent death, myocardial infarct and coronary revascularization.1 This study reports the prevalence and characteristics of patients with MSIMI vs. exercise stress induced myocardial ischemia (ESIMI) and CHD from the REMIT (The Responses of Mental Stress Induced Myocardial Ischemia to Escitalopram Treatment) study, a National Heart, Lung, and Blood Institute (NHLBI) sponsored prospective, randomized, double-blind, placebo-controlled study (NCT00574847) designed to assess the efficacy of escitalopram on MSIMI in patients with CHD(2). The primary endpoint of REMIT (yet to be reported) will be the improvement, worsening or no change in MSIMI at the end of six weeks of treatment.
Methods
Patients were male and female adults with a history of known CHD by any of the following criteria:
- ≥70% stenosis on coronary angiography
- history of myocardial infarction
- history of prior revascularization with either coronary artery bypass graft (CABG) surgery or percutaneous coronary intervention (PCI)
Patients underwent mental stress and exercise stress test testing. Mental stress tasks included:
- mental arithmetic
- public speaking with anger recall
- mirror trace
There was a rest period of six minutes after each mental stress test. After mental stress testing, patients underwent a treadmill exercise stress test using standard Bruce protocol.
Myocardial ischemia assessment was done using echocardiography and electrocardiography (ECG). Echocardiography was obtained during the last three minutes of baseline resting period, during each mental stress test and at the peak of exercise testing for three minutes. MSIMI is defined by any of the following compared to rest:
- any development or worsening of wall motion
- reduction of left ventricular ejection fraction (LVEF) ≥ 8%
- deviation (depression or elevation) of ECG ST-segment in two or more leads lasting ≥ three consecutive beats occurring during at least one of the three mental stress tests
The specific focus of this study was to examine the prevalence and demographic/clinical characteristics of MSIMI, as well as compare left ventricular responses to mental and exercise stress tests.
Results
Exactly 400 patients provided consent for baseline assessments of which 310 patients underwent stress testing. The most common reasons for exclusion were un-interpretable stress test images and patients being on antidepressants that could not be discontinued.
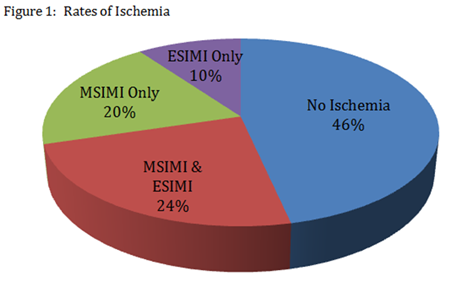
 Selected patient characteristics are listed in Table 1. MSIMI was observed more often versus ESIMI (44% vs. 34%, p=0.003). 47% of patients had no ischemia during any stress test, 24% showed both MSIMI and ESIMI, 20% had MSIMI only and 10% had ESIMI only (Figure 1). MSIMI induced greater rates of wall motion abnormalities (36% vs. 22%, p=0.0001) and LVEF reduction ≥8% (18% vs. 5%, p < 0.0001). Zero patients with MSIMI exhibited ischemic ECG changes. Exercise capacity was not different between patients with and without MSIMI.
Selected patient characteristics are listed in Table 1. MSIMI was observed more often versus ESIMI (44% vs. 34%, p=0.003). 47% of patients had no ischemia during any stress test, 24% showed both MSIMI and ESIMI, 20% had MSIMI only and 10% had ESIMI only (Figure 1). MSIMI induced greater rates of wall motion abnormalities (36% vs. 22%, p=0.0001) and LVEF reduction ≥8% (18% vs. 5%, p < 0.0001). Zero patients with MSIMI exhibited ischemic ECG changes. Exercise capacity was not different between patients with and without MSIMI.
A few patient subtypes, in univariate analysis, exhibited a higher incidence of MSIMI: women (OR 1.88 95% CI 1.04 to 3.42, p = 0.04], unmarried patients (OR 1.99, 95% CI 1.19 to 3.36, p=0.009) and those who lived alone (OR: 2.24, 95% CI 1.19 to 4.20, p=0.01). However, none of these individual characteristics showed independent association in multivariate analysis. The investigators created new variables to account for intercorrelations of the variables composed of gender/marital status or gender/living situation. Logistic regression analysis showed that unmarried men (OR 2.57, 95% CI 1.33 to 4.97, p=0.005) and married women (OR 3.18, 95% CI 1.22 to 8.32 p=0.02) when compared to married men were more likely to show MSIMI. In addition, men and women living alone when compared to men living with someone were more likely to show MSIMI. None of these factors were associated with an increased incidence of ESIMI.
 Physical symptoms between those with MSIMI and ESIMI were different. Patients with MSIMI rarely exhibited chest pain (2%) or dyspnea (4%) while patients with ESIMI exhibited higher rates of chest pain (21%) or dyspnea (61%).
Physical symptoms between those with MSIMI and ESIMI were different. Patients with MSIMI rarely exhibited chest pain (2%) or dyspnea (4%) while patients with ESIMI exhibited higher rates of chest pain (21%) or dyspnea (61%).
Conclusions
The investigators conclude that: 1) MSIMI was seen more commonly than ESIMI and occurred in patients with and without ESIMI. 2) MSIMI rate was different in men and women, particularly when considering marital and living status. The investigators further state that women, unmarried men and individuals living alone are at higher risk for MSIMI.
Commentary/Perspective
As early as 1950, Harold Wolff in the first issue of Circulation recognized the potential link between cardiac disease and stress.3 Mental stress, a particularly common patient complaint, is probably underrecognized as a risk factor for cardiac ischemia by clinicians. Given an increased risk for adverse outcomes in the setting of MSIMI, how best can we advise and manage our patients when it comes to mental stress? Should mental stress be approached as similarly as other more traditional risk factors such as hypertension, hyperlipidemia, and smoking? Are clinicians equipped with an adequate evidence base to effectively recognize and treat mental stress ischemia? Given a dearth of large studies on this issue, the article of the month from Jiang, et al. provides an important prospective examination on the prevalence of MSIMI.4
In particular, the authors observe that there may be increased prevalence of MSIMI in women, unmarried men and individuals living alone. While this finding raises interesting questions, it is unclear whether these subgroups, through this exploratory analysis from a relatively small patient sample, are truly at higher risk for MSIMI. For example, women only constituted only 17% of the study population and are underrepresented relative to the general population. At the same time, Bairey Merz, et al. found that women had greater blood pressure, heart rate and rate-pressure product responses to mental stress with an accentuated difference in post-menopausal women that may support a physiologic basis for MSIMI in women.5 The extent of psychosocial and biological interactions that may lead women, unmarried men and individuals living alone and perhaps other specific subgroups require further study.
Another area of interest from Jiang, et al. involves the optimal method of detecting MSIMI given the relative absence of physical symptoms in MSIMI of chest pain (2%) and dyspnea (4%). In one study, in the presence of coronary disease, mental stress was shown to demonstrate ischemia in activities of daily life by holter monitor6 representing a potential method of detection. In a research environment, a personally relevant emotionally arousing speaking task has been shown to induce greater wall motion abnormalities than less specific cognitive tasks.7 However, this methodology is rarely employed in clinician’s offices. As MSIMI may present silently, the role of routine exercise stress testing, such as used in the study from Jiang, et al. however, also remains unclear.
From recognition of MSIMI to mechanism, several potential theories have been posited as causes of MSIMI. One possibility from animal models is that coronary constriction or endothelial injury is mediated by neuro hormones from specific neuro-cortical activation.8 Coronary angiography performed during mental stress activities has shown coronary vasoconstriction in diseased segments, though the degree of effect has been variable.9 The role of catecholamine release has been variable in its association with MSIMI with both positive and negative correlations.
Thus, a full understanding of treatment options of MSIMI remains inadequate. The use of beta-blockade and calcium channel blockade has been studied on a limited basis and found to have no benefit, probably reflecting the mixed effects of catecholamine release on MSIMI.10 However, the use of psycho-behavioral intervention, including an aerobic exercise and stress management program has been shown to have a significant benefit suggesting that reducing negative emotions may be a key therapeutic approach.11 Heightened platelet aggregation noted in diseases states such as acute coronary syndromes may also play a role in depression and MSIMI. As several studies have shown that SSRIs may reduce platelet activity,12 upcoming results from the REMIT trial will examine whether SSRI treatment will result in decreased MSIMI.
As findings from this study from Jiang, et al. begin to give us clearer insights on exactly which groups of patients may be at higher risk for MSIMI, further randomized prospective trials are needed for refined answers on appropriate methodology to recognize and treat MSIMI. While modifying traditional risk factors will continue to have considerable importance in disease prevention, a reasoned clinical response to MSIMI best appears to be a multifaceted one with the cardiologist as a central figure. For now, the current evidence base and practical clinical judgment supports encouraging patients to seek ways to modify their mental stress through psychotherapy, exercise, stress management training and seeking support in friends and family.11
References
- Strike PC, Steptoe A. Systematic review of mental stress-induced myocardial ischaemia. Eur Heart J 2003;24:690-703.
- Jiang W, Velazquez EJ, Samad Z et al. Responses of mental stress-induced myocardial ischemia to escitalopram treatment: background, design, and method for the Responses of Mental Stress Induced Myocardial Ischemia to Escitalopram Treatment trial. Am Heart J 2012;163:20-6.
- Wolff HG. Life stress and cardiovascular disorders. Circulation 1950;1:187-203.
- Jiang W, Samad Z, Boyle S et al. Prevalence and clinical characteristics of mental stress-induced myocardial ischemia in patients with coronary heart disease. J Am Coll Cardiol 2013;61:714-22.
- Bairey Merz CN, Kop W, Krantz DS, Helmers KF, Berman DS, Rozanski A. Cardiovascular stress response and coronary artery disease: evidence of an adverse postmenopausal effect in women. Am Heart J 1998;135:881-7.
- Gabbay FH, Krantz DS, Kop WJ et al. Triggers of myocardial ischemia during daily life in patients with coronary artery disease: physical and mental activities, anger and smoking. J Am Coll Cardiol 1996;27:585-92.
- Rozanski A, Bairey CN, Krantz DS et al. Mental stress and the induction of silent myocardial ischemia in patients with coronary artery disease. N Engl J Med 1988;318:1005-12.
- Rozanski A, Blumenthal JA, Kaplan J. Impact of psychological factors on the pathogenesis of cardiovascular disease and implications for therapy. Circulation 1999;99:2192-217.
- Yeung AC, Vekshtein VI, Krantz DS et al. The effect of atherosclerosis on the vasomotor response of coronary arteries to mental stress. N Engl J Med 1991;325:1551-6.
- Andrews TC, Parker JD, Jacobs S et al. Effects of therapy with nifedipine GITS or atenolol on mental stress-induced ischemic left ventricular dysfunction. J Am Coll Cardiol 1998;32:1680-6.
- Blumenthal JA, Sherwood A, Babyak MA et al. Effects of exercise and stress management training on markers of cardiovascular risk in patients with ischemic heart disease: a randomized controlled trial. JAMA 2005;293:1626-34.
- Pollock BG, Laghrissi-Thode F, Wagner WR. Evaluation of platelet activation in depressed patients with ischemic heart disease after paroxetine or nortriptyline treatment. J Clin Psychopharmacology 2000;20:137-40.
Clinical Topics: Atherosclerotic Disease (CAD/PAD)
Keywords: Citalopram, Coronary Artery Disease, Coronary Disease, Myocardial Infarction, Myocardial Ischemia
< Back to Listings