"Can We Clip It?": A Review of TEER in the Adult Congenital Heart Disease Population
Quick Takes
- Atrioventricular valvular regurgitation (AVVR) is associated with significant morbidity and mortality in patients with adult congenital heart disease (ACHD).
- Transcatheter edge-to-edge repair (TEER) is an attractive therapy in patients with AVVR who are at high surgical risk.
- TEER requires careful patient selection, preprocedural planning, and collaboration between procedural and imaging experts in both acquired and congenital heart disease to be successfully implemented in the ACHD population.
Atrioventricular valvular regurgitation (AVVR) is commonly seen in adults with congenital heart disease (ACHD), including those with congenitally corrected transposition of the great arteries (ccTGA), atrial switch correction for dextro-transposition of the great arteries (d-TGA), atrioventricular (AV) canal defect, and single-ventricle Fontan circulation. Significant AVVR is associated with heart failure (HF), end-organ dysfunction, and death.1 Surgical correction of AVVR, for which valve repair is preferred over valve replacement in the setting of congenital heart disease (CHD), is often high risk because of repeat sternotomies, vulnerable myocardial mechanics (especially those with right ventricular morphology), and the difficulty of sustaining a durable repair.2 In patients with prohibitive surgical risk, heart transplant is often the only option. Thus, percutaneous transcatheter therapies are emerging as options in the treatment of AVVR. Although transcatheter valve-in-valve replacement is a well-explored approach for patients with prior annuloplasty rings and bioprosthetic valves in situ, options for those with native atrioventricular valves (AVVs) include transcatheter edge-to-edge repair (TEER), percutaneous annuloplasty, and percutaneous tricuspid valve (TV) replacement.3 Of these options, TEER has been extensively studied and performed in patients with acquired heart disease, and has been shown to be an effective treatment in adult patients with severe symptomatic mitral regurgitation (MR) and tricuspid regurgitation (TR) and high surgical risk.4,5 As the applications of TEER have become more refined in adults with both functional and degenerative valvular regurgitation, there has been a growing interest in applying TEER technologies to patients with CHD.
There are 3 TEER device platforms currently available in the United States and approved for use in adult patients: the MitraClip (Abbott Laboratories) and PASCAL/ACE (Edwards Lifesciences) for TEER of the mitral valve, and the TriClip (Abbott Laboratories) for TEER of the TV (Figure 1). Both the MitraClip and TriClip systems use the same TEER clips, which come in four sizes of differing width and arm length. They differ in their steerable delivery systems, with dedicated axes of maneuverability to aid in working in the left atrium (MitraClip) and right atrium (TriClip). The PASCAL/ACE system differs in its nitinol design and use of a spacer in the implant itself (with a larger spacer in the 10 mm PASCAL than in the 6 mm ACE device), potentially reducing stress on the AVV leaflets after repair. Each system allows independent grasping of the valve leaflets, after which small maneuvers can be made to optimize the degree of coaptation and residual valvular regurgitation before deploying the clip. As these devices were designed for acquired heart disease, their adaptation in CHD presents unique challenges; large clefts may preclude adequate leaflet grasping with available clip sizes, and maneuverability through surgical baffles may be difficult. Concerns have also been raised about the ability to surgically repair an AVV after failed TEER, sometimes necessitating valve replacement.6 More generally speaking, the decision to pursue a transcatheter intervention as opposed to referral for advanced HF therapies should also be carefully weighed, as some authors have suggested that these interventions can delay timely referral for transplant.7
Figure 1: Current Commercially Available TEER Implants
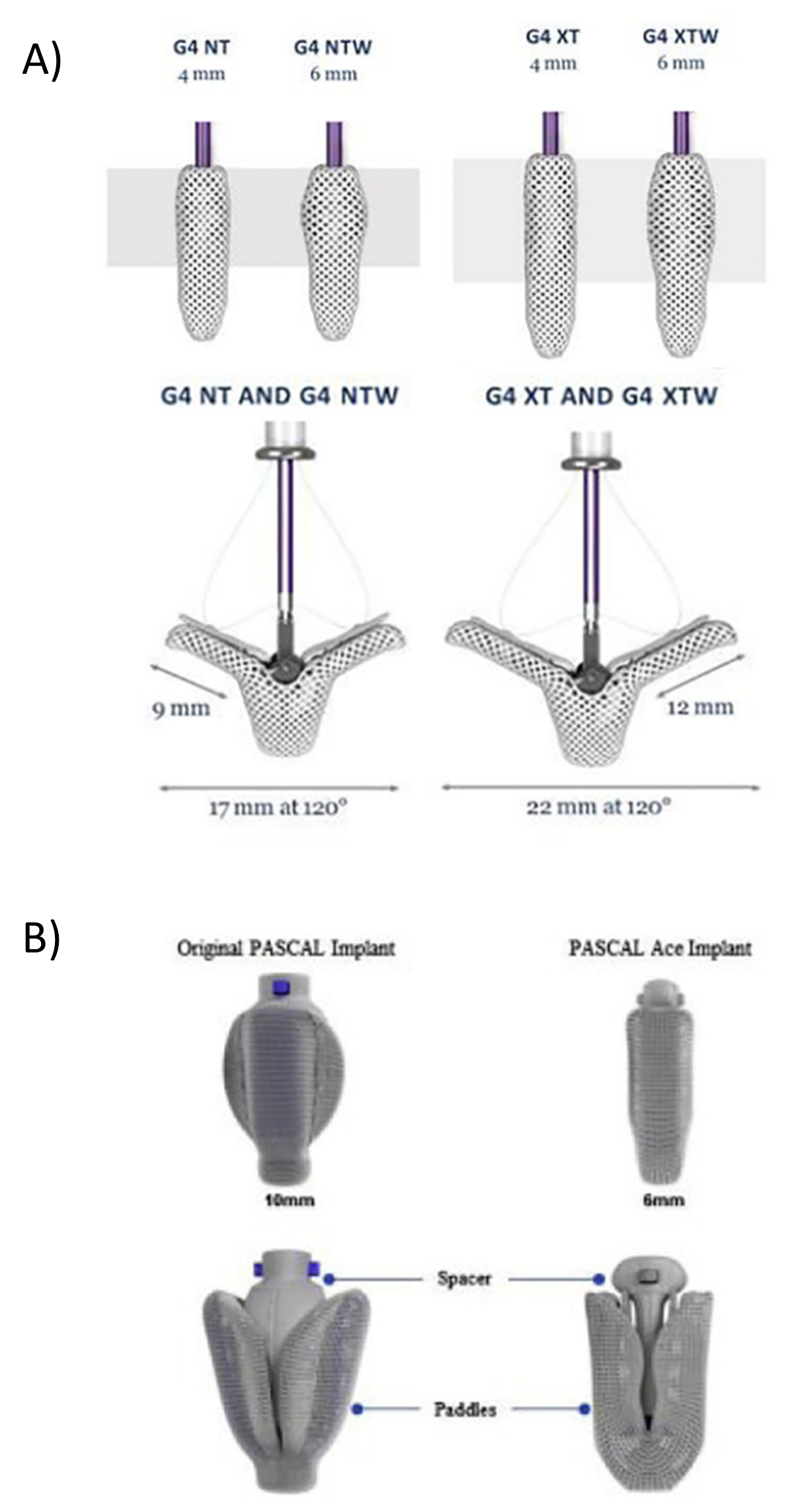
Reprinted with permission from Webb JG, Boone RH. Mitral Transcatheter Edge-to-Edge Repair: A Choice! JACC Cardiovasc Interv. 2022;15(24):2537-2540. doi:10.1016/j.jcin.2022.10.005
(Panel A) The MitraClip/TriClip implants (Abbott Laboratories), which come in four sizes of variable length and width. (Panel B) The PASCAL/ACE implants (Edwards Lifesciences), which differ in paddle and spacer size.
TEER = transcatheter edge-to-edge repair.
Although a detailed analysis of the randomized trials that led to the approval of these devices is beyond the scope of this review, it is important to acknowledge some of the current controversies in the TEER space. Two major trials of mitral TEER in patients with HF and functional MR showed conflicting results, with the COAPT (Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients with Functional Mitral Regurgitation) trial data demonstrating lower rates of HF hospitalization and death in the device group and the MITRA-FR (Percutaneous Repair With the MitraClip Device for Severe Functional/Secondary Mitral Regurgitation) trial data showing no difference in all-cause mortality or HF hospitalization. One widely proposed explanation is that the patients who derived benefit from TEER in the COAPT trial had a degree of MR out of proportion to their underlying cardiomyopathy, emphasizing the role of careful patient selection in successful TEER. Trial results have also demonstrated that mitral TEER is effective at reducing degenerative MR, but the durability of the results is still being studied and a head-to-head comparison with surgical results is still in trial.8,9 To date, there has been one trial of a dedicated TEER device in severe symptomatic TR, which demonstrated an improvement in patient-reported quality-of-life scores, without differences in mortality, TV surgery, or HF hospitalization.10 Importantly, these randomized trials did not include patients with complex CHD.
Careful and thorough preprocedural planning is crucial before embarking on TEER in an adult patient with CHD. Transesophageal echocardiogram performed by an experienced ACHD specialist familiar with structural intervention is necessary to understand the nuances of AVV anatomy, the various etiologies of AVVR, and the anatomical views needed to assess potential case complexity to determine optimal patients for this technology. Cross-sectional imaging including three-dimensional printing and virtual reality simulation is also key in examining the catheter course from the femoral venous vasculature to delineate the optimal transbaffle or trans-septal puncture site (for systemic AVVs) and in positioning the device at the valve of interest (Table 1). A multidisciplinary approach from patient selection to examining technical feasibility and candidacy is critical. Preprocedural invasive hemodynamic evaluation is frequently needed to guide clinical decision-making when performing the procedure, such as closing the baffle/septal puncture site. The multidisciplinary team planning and performing this procedure includes an interventional echocardiography specialist with deep understanding of CHD valve anatomy and hemodynamics, an interventional cardiologist with expertise in TEER in adult patients without CHD in addition to CHD knowledge, and ACHD board-certified cardiologists and CHD surgeons.
Table 1: Considerations For TEER in CHD Patients
| Common CHD indications | ccTGA, atrial switch for d-TGA, single-ventricle anatomy, AV canal defect |
| TEER devices | MitraClip,a TriClip,a PASCALb |
| Mechanism of action | Clip-based coaptation enhancement of AVV leaflets |
| Challenges in CHD | Large clefts, abnormal AVV morphology, difficulty with transbaffle puncture, insurance and payer approval |
| Preprocedural evaluation | TEE for anatomy, invasive hemodynamics, cross-sectional imaging (CMR, CT), 3D printing, virtual simulation |
| Outcomes in ACHD | Case reports show feasibility; long-term efficacy remains unclear |
| Future directions | Need for specialized ACHD expertise, surgical backup, improved device adaptation |
a Product of Abbott Laboratories.
b Product of Edwards Lifesciences.
3D = three-dimensional; ACHD = adult congenital heart disease; AVV = atrioventricular valve; ccTGA = congenitally corrected transposition of the great arteries; CHD = congenital heart disease; CMR = cardiac magnetic resonance; CT = computed tomography; d-TGA = dextro-transposition of the great arteries; TEE = transesophageal echocardiogram.
There have been several case series and reports demonstrating success of TEER in complex forms of CHD, including hypoplastic left heart syndrome palliated with a Fontan, complete AV canal defect, d-TGA after an atrial switch, and ccTGA.11 These reports show the promise of TEER, and professional societies have shown interest in growing access to this technology in the CHD population.12 The decision to pursue TEER should only be made for carefully selected patients, in centers with imaging and procedural expertise, and as surgical backup to address potential complications; however, in the right setting, TEER is feasible in complex CHD cases and represents an exciting emerging technology for addressing AVVR in adult patients with CHD.
References
- Abdelrehim AA, Stephens EH, Miranda WR, et al. Systemic atrioventricular valve surgery in patients with congenitally corrected transposition of the great vessels. J Am Coll Cardiol. 2023;82(23):2197-2208. doi:10.1016/j.jacc.2023.09.822
- Kadowaki S, Venet M, Tocharoenchok T, et al. Are we getting better?: Ongoing challenges of atrioventricular valve repair in children with single ventricle physiology. J Am Heart Assoc. 2025;14(9):e037348. doi:10.1161/JAHA.124.037348
- Barry OM, Bouhout I, Kodali SK, et al. Interventions for congenital atrioventricular valve dysfunction: JACC focus seminar. J Am Coll Cardiol. 2022;79(22):2259-2269. doi:10.1016/j.jacc.2021.08.083
- Writing Committee Members, Otto CM, Nishimura RA, et al. 2020 ACC/AHA guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2021;77(4):e25-e197. doi:10.1016/j.jacc.2020.11.018
- Arnautovic JZ, Ya'Qoub L, Wajid Z, et al. Outcomes and complications of mitral and tricuspid transcatheter edge-to-edge repair. Interv Cardiol. 2024;19:e20. Published 2024 Oct 28. doi:10.15420/icr.2024.08
- Chikwe J, O'Gara P, Fremes S, et al. Mitral surgery after transcatheter edge-to-edge repair: Society of Thoracic Surgeons database analysis. J Am Coll Cardiol. 2021;78(1):1-9. doi:10.1016/j.jacc.2021.04.062
- Egbe AC, Miranda WR, Jain CC, et al. Incidence and outcomes of advanced heart failure in adults with congenital heart disease. Circ Heart Fail. 2022;15(12):e009675. doi:10.1161/CIRCHEARTFAILURE.122.009675
- McCarthy PM, Whisenant B, Asgar AW, et al. Percutaneous MitraClip device or surgical mitral valve repair in patients with primary mitral regurgitation who are candidates for surgery: design and rationale of the REPAIR MR trial. J Am Heart Assoc. 2023;12(4):e027504. doi:10.1161/JAHA.122.027504
- Annetine Gelijns, Icahn School of Medicine at Mount Sinai. Percutaneous or Surgical Repair In Mitral Prolapse And Regurgitation for ≥60 Year-olds (PRIMARY) (ClinicalTrials website). 2025. Available at: https://clinicaltrials.gov/study/NCT05051033. Accessed 09/15/2025.
- Sorajja P, Whisenant B, Hamid N, et al. Transcatheter repair for patients with tricuspid regurgitation. N Engl J Med. 2023;388(20):1833-1842. doi:10.1056/NEJMoa2300525
- Alshawabkeh L, Mahmud E, Reeves R. Percutaneous mitral valve repair in adults with congenital heart disease: report of the first case-series. Catheter Cardiovasc Interv. 2021;97(3):542-548. doi:10.1002/ccd.29238
- Salavitabar A, Al-Ahmadi M, Eng MH, et al. Transcatheter atrioventricular valve repair and replacement technologies in pediatric and adult congenital heart disease: a paradigm for improving access. J Soc Cardiovasc Angiogr Interv. 2024;3(12):102398. Published 2024 Dec 19. doi:10.1016/j.jscai.2024.102398
Clinical Topics: Congenital Heart Disease and Pediatric Cardiology, Congenital Heart Disease, Invasive Cardiovascular Angiography and Intervention, Heart Failure and Cardiomyopathies, Valvular Heart Disease
Keywords: Heart Defects, Congenital