New Research Adds to Growing Evidence Surrounding Lp(a), Including Global Prevalence
New original research – part of a special JACC focus issue on lipids – adds to the growing body of evidence surrounding lipoprotein(a) (Lp[a]) and its contribution as an independent causal risk factor for cardiovascular disease and aortic stenosis.
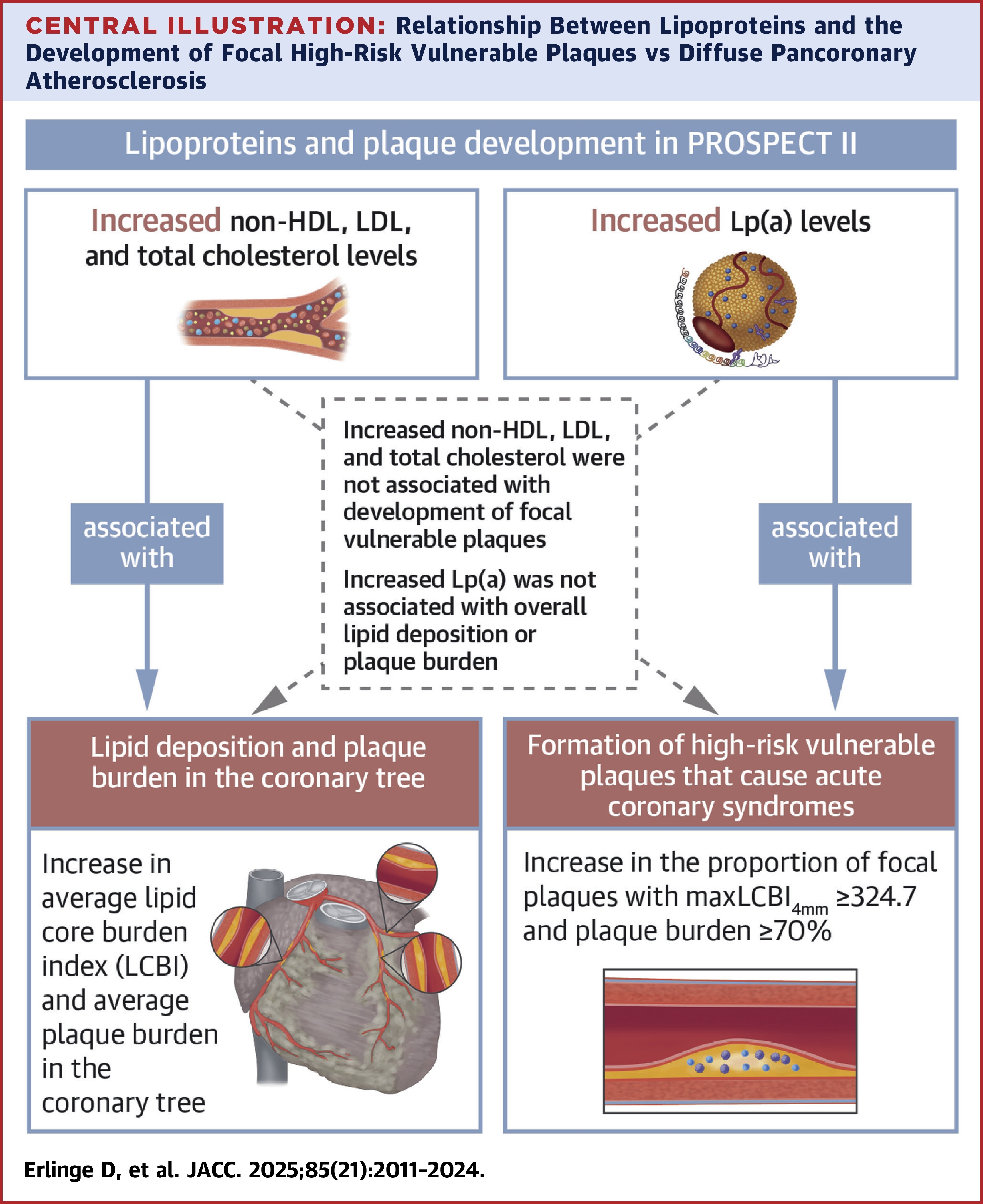
In a substudy of the PROSPECT II trial, researchers evaluated the relationships between Lp(a), total cholesterol, LDL-C, non–HDL-C and triglycerides to pancoronary plaque volume, pancoronary lipid core burden index (LCBI) and the presence of focal vulnerable plaques in 865 patients. Using multivariable analysis, David Erlinge, MD, PhD, FACC, et al., found that elevated total cholesterol, LDL-C and non–HDL-C, but not Lp(a), were strongly associated with pancoronary atherosclerosis and lipid deposition. However, elevated Lp(a) was strongly associated with the presence of focal vulnerable plaques.
"These findings may explain the association between high Lp(a) levels and future myocardial infarction and suggest a unique role for Lp(a) in atherosclerosis progression and plaque vulnerability," says Erlinge and colleagues.
According to the study investigators, the "findings warrant dedicated imaging studies in patients treated with Lp(a)-lowering agents to assess which components of plaque composition are most affected." They also suggest large-scale outcomes trials to test the hypothesis that combination treatment with agents that both lower LDL-C and Lp(a) might have synergistic clinical benefits" in reducing both intermediate- and long-term major adverse cardiovascular events.
In a related editorial comment, Seong-Bong Wee, MD, et al., highlight the "dawn of a new era in assessment and management of vulnerable plaque," while also noting that substantial knowledge gaps remain in terms of identification, diagnosis and optimal management. They write: "Future efforts should focus on refining the definition of high-risk vulnerable plaques and improving their detection using both noninvasive and invasive imaging modalities, aided by evolving technologies as well as by the detection of candidate biomarkers for reliable assessment of coronary plaque vulnerability.
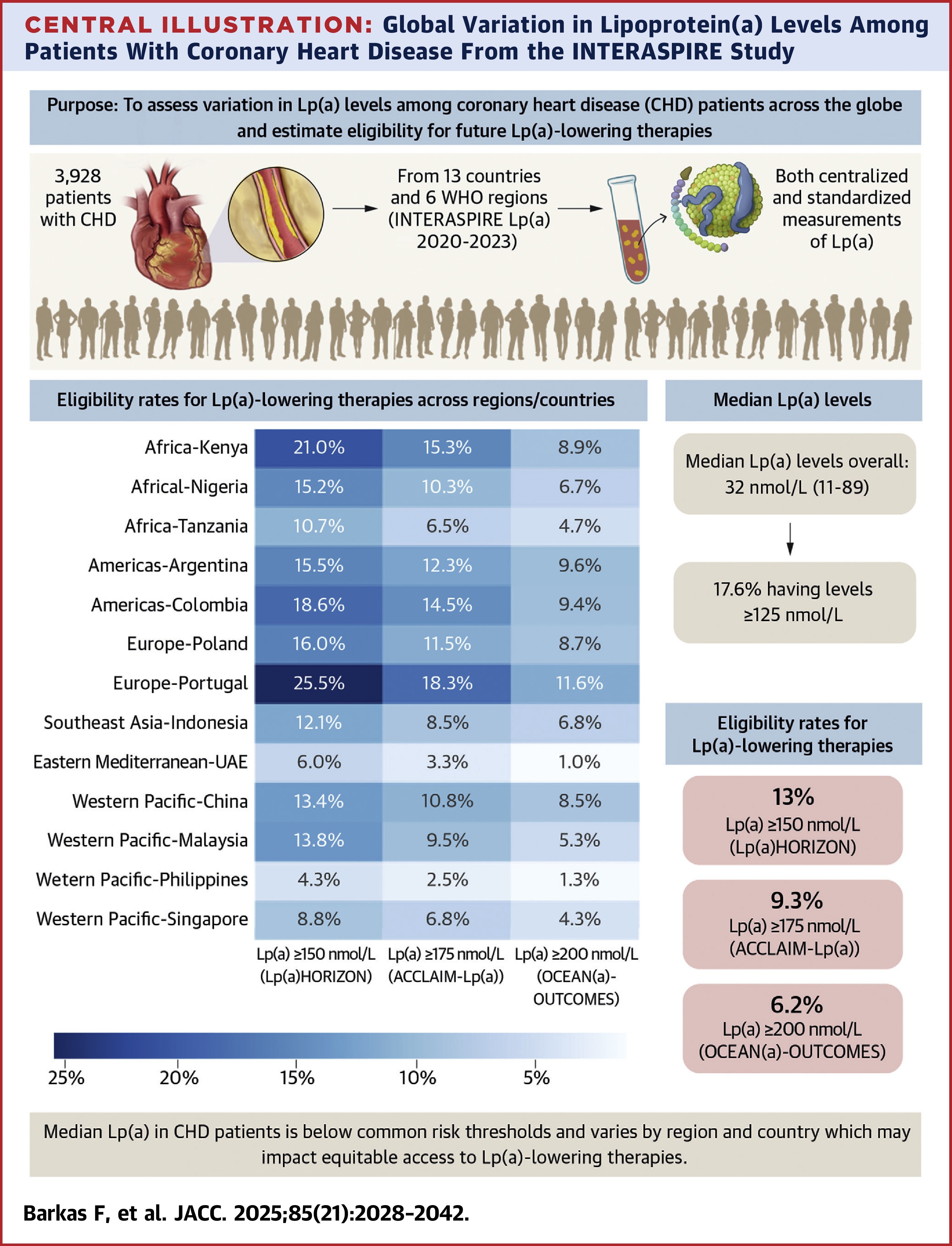
A second study assessing Lp(a) levels in patients with coronary heart disease (CHD) in 13 countries spanning six geographical regions found significant variation across countries and regions. While the overall median Lp(a) was 32 nmol/L, median levels were highest in Africa (62 nmol/L) and lowest in Western Pacific (22 nmol/L). There was also wide variation between countries within the same regions. For example, within Europe median levels in Portugal were 59 nmol/L compared with Poland at 19.5 nmol/L, while in South America median levels in Colombia were 46 nmol/L compared with Argentina at 32 nmol/L.
Among the patients enrolled in the study, 13% had Lp(a) >150 nmol/L, 9.3% had Lp(a) >175 nmol/L and 6.2% had Lp(a) >200 nmol/L, making them eligible for Lp(a)-lowering therapies. However, similar with median levels, eligibility rates varied widely by country, with eligibility greatest in Portugal and lowest in the Philippines. Of note, "the vast majority" of patients had Lp(a) levels far below the "typical risk-enhancing threshold," according to study authors Fotios Barkas, MD, PhD, et al. This suggests "that the attributable risk from Lp(a) is more complex than previously perceived," they said.
In other findings, most patients with elevated Lp(a) had poorly controlled levels of traditional risk factors, meaning "if emerging Lp(a)-lowering therapies are unavailable in some countries, traditional risk factor management needs to improve several-fold to offset the residual risk from high Lp(a)," says Barkas and colleagues. They also caution that the significant geographical variations could "likely impact equitable access to emerging therapies should they demonstrate clinical benefit."
In a related editorial comment, Ron Blankstein, MD, FACC, et al., praised the authors for their work, noting that "unlike previous studies that have historically relied on nonuniform assays or ethnically pooled data, the present work helps elucidate geographic and ethnic variability in Lp(a) levels, findings that have implications for both attributable risk as well as the role that future Lp(a)-directed therapies may play in the landscape of secondary prevention across the globe." They go on to say: "Future research must clarify not only who is at risk but also who stands to benefit most – ensuring that scientific progress translates into personalized cardiovascular care worldwide."
Citations:
- Erlinge, D, Tsimikas, S, Maeng, M. et al. Lipoprotein(a), Cholesterol, Triglyceride Levels, and Vulnerable Coronary Plaques: A PROSPECT II Substudy. JACC. 2025 Jun, 85 (21) 2011–2024. doi: 10.1016/j.jacc.2025.04.013
- Barkas, F, Brandts, J, De Bacquer, D. et al. Global Variation in Lipoprotein(a) Levels Among Patients With Coronary Heart Disease: Insights From the INTERASPIRE Study and Implications for Emerging Lp(a)-Lowering Therapies. JACC. 2025 Jun, 85 (21) 2028–2042. doi:10.1016/j.jacc.2025.04.010
Clinical Topics: Diabetes and Cardiometabolic Disease, Dyslipidemia, Valvular Heart Disease, Advanced Lipid Testing, Hypertriglyceridemia, Lipid Metabolism, Nonstatins
Keywords: Aortic Valve Stenosis, Cardiovascular Diseases, Coronary Disease, Risk Factors, Atherosclerosis, Cholesterol, LDL, Triglycerides, Lipoprotein(a)
< Back to Listings