Is Same-Day Discharge Safe After M-TEER?
Same-day discharge (SDD) following mitral transcatheter edge-to-edge repair (M-TEER) was found to be uncommon, but compared with next-day discharge (NDD) it was associated with a similar risk of 90-day readmission and lower costs for the index hospitalization, according to research presented April 25 at the SCAI 2026 Scientific Sessions & CAIC-ACCI Summit and simultaneously published in JACC: Advances.
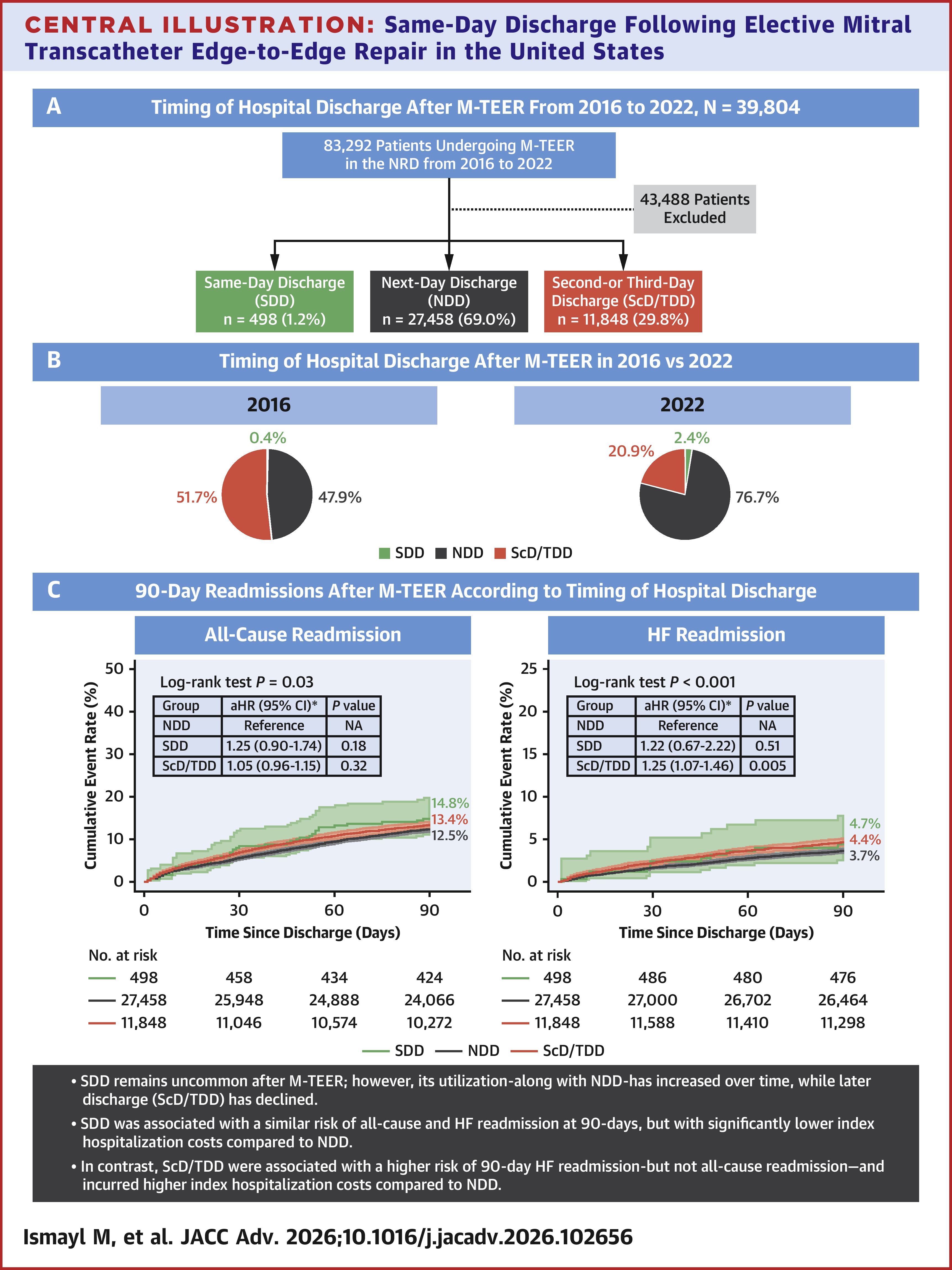
In their review of the Nationwide Readmissions Database (2016-2022), Mahmoud Ismayl, MD, and colleagues identified 39,804 weighted hospitalizations for M-TEER: 1.2% (n=498) involved SDD; 69.0% (n=27,458) involved NDD and 29.8% (n=11,848) involved second- or third-day discharge (ScD/TDD). The patients were about 78 years old and about 44% were women.
Results showed SDD, when compared with NDD, was associated with a similar risk of 90-day readmission, both for all causes (14.8% vs. 12.5%; adjusted hazard ratio [aHR], 1.25) and heart failure (HF; 4.4% vs. 3.7%; aHR, 1.22) and significantly lower index hospitalization costs ($38,029 vs. $43,319; p=0.03). ScD/TDD, on the other hand, was associated with a higher risk of 90-day HF (but not all-cause) readmission and higher index hospitalization costs compared with NDD ($49,648 vs. $43,319; p<0.001).
Between 2016 and 2022, the proportion of SDDs and NDDs also increased, from 0.4% to 2.4% and 47.9% to 76.7%, respectively, while ScD/TDDs decreased from 51.7% to 20.9% (all ptrend <0.001).
Major bleeding complications, history of chronic pulmonary disease or renal failure, and nonhome discharge were all associated with lower likelihood of SDD, while major bleeding complications, female sex, and a history of HF, atrial fibrillation, renal failure, hemodialysis dependence, liver disease, chronic pulmonary disease or cancer were all independent predictors of higher 90-day all-cause readmission following M-TEER.
Patients with SDD were more frequently hospitalized in urban teaching hospitals with greater bed capacity and were more likely to reside in neighborhoods within the lowest quartile of median household income, raising additional questions about the observed socioeconomic differences.
"As operators increasingly adopt SDD – particularly at high-volume, resource-optimized centers – its broader implementation in the M-TEER population warrants thoughtful evaluation," write Ismayl and colleagues. "Developing standardized criteria for SDD eligibility – potentially incorporating frailty scores, access site characteristics, procedural success, degree of residual [mitral regurgitation], and early recovery indicators – will be essential to ensure patient safety."
Clinical Topics: Valvular Heart Disease, Mitral Regurgitation
Keywords: Mitral Valve Insufficiency, Patient Readmission, Patient Discharge
< Back to Listings