Cover Story | A New Threat to Cardiovascular Health: Climate Change, Extreme Weather and Wildfires

The increasing frequency and intensity of extreme weather events and wildfires, driven by climate change, pose a growing threat to cardiovascular health. This was starkly illustrated in January 2025 when seven major wildfires struck Los Angeles County simultaneously, forcing more than 200,000 residents to evacuate and creating severe air quality challenges across one of America's largest metropolitan areas. Recent research provides mounting evidence that these environmental stressors impact heart health in both the short- and long-term.
California Wildfires Take Toll
The catastrophic wildfires that struck Los Angeles County in January highlight the growing cardiovascular health threats facing urban populations. A series of seven major fires, most notably the Eaton and Palisades fires, forced tens of thousands of residents to evacuate and burned more than 57,000 acres.
The fires, driven by hurricane-force Santa Ana winds, were intensified by severe drought conditions. Southern California had experienced its driest start to the rainy season and driest nine-month period on record, leaving vegetation dangerously dry.
Their occurrence in winter, rather than during traditional fire season, exemplifies how climate change is altering wildfire patterns. Based on findings from previous California wildfire studies, such events likely posed significant cardiovascular risks, particularly for vulnerable populations with preexisting heart conditions.
Janet Wei, MD, FACC, was at the center of it all in her role as a cardiologist at Cedars-Sinai Medical Center. "We had many staff members who were evacuated or lost their homes, and patient care was definitely affected," she says. Wei is currently the governor of the Southern California ACC Chapter.
Cedars-Sinai postponed nonemergent procedures for a few days due to the Palisades fire, which was close to its main medical center and the Marina del Rey campus. The system also closed several outpatient offices in evacuation areas, along with some offices outside of evacuation areas affected by power outages or other weather-related challenges.
Patients were directed to Cedars-Sinai's social media sites for basic instructions on masking and monitoring air quality. "We received a flurry of questions from patients about how the fires might affect their cardiovascular health and what they can do to protect themselves," says Wei. Some patients chose to leave the area and visit family in other parts of the country.
Beyond the numerous logistical challenges – including the sudden need for virtual consultations and emergency prescription refills – there was also the added stress. "We heard stories of individuals who had to abandon their cars on the roadside to escape the fires. Some patients experienced emotional stress-induced angina, even if they did not present with a full-blown acute coronary syndrome."
Overall, patients appeared eager to follow advice on masking and using air filtration in their homes and workplaces. In fact, the U.S. air purifier market is expected to grow from 4.54 billion in 2024 to 6.82 billion by 2030, in large part due to air pollution, according to a recent Research and Markets report.1
To help California clinicians better advise their patients and screen for various cardiovascular issues related to these extreme events, the Southern California ACC Chapter organized a series of webinars, the first of which was in early March.
Visit CAACC.org to view the webinar series from the Southern California ACC Chapter.
"When the fires were burning, our patients had important questions and issues about smoke and air quality that we needed to be prepared to address. There are still many factors to consider regarding smoke residues, toxins in the air and water supply, contaminated water in swimming pools, and, of course, how to prepare for the next time," says Wei.
Wildfire Air Pollution and CV Risk
Wildfire smoke contains fine particulate matter (PM2.5), which penetrates deep into the lungs, triggering systemic inflammation, oxidative stress and vascular dysfunction. While PM2.5 exposure has been linked to adverse cardiovascular outcomes, the association of wildfire-related PM2.5 and cardiovascular health outcomes has been inconsistent.
Jamal S. Rana, MD, PhD, FACC, chair of medical specialties at Kaiser Permanente's Oakland Medical Center and immediate past governor of ACC's Northern California Chapter, along with Stacey E. Alexeeff, PhD, a research scientist at the Kaiser Permanente Northern California Division of Research, have been studying the cardiovascular effects of wildfire air pollution during two major California wildfires in 2018.
In a recently published paper, they report that exposure to high levels of fine PM2.5 from wildfires was associated with increased rates of cardiovascular events and death, though the relationship was complex.2
Each fire burned more than 100,000 acres, with smoke plumes extending hundreds of miles. The Mendocino Complex fires burned for nearly all of July and August 2018, creating smoke conditions that lasted 26-51 days across different counties. In contrast, the Camp fire, which broke out in November, was contained more quickly, producing smoke conditions that lasted 11-15 days depending on the county.
During the Mendocino Complex wildfire, high PM2.5 concentrations were linked to a 23.1% increase in cardiovascular events and a 35.8% increase in mortality compared to periods with good air quality. However, during the later Camp Fire, despite having some of the world's highest PM2.5 levels, researchers did not observe increased cardiovascular risk.
Their retrospective cohort study was conducted within Kaiser Permanente Northern California, which includes 3.2 million adults (≥18 years old) enrollees, residents of 35 counties in Northern California.
The authors note that public awareness and protective behaviors may explain the lack of increased cardiovascular disease risk in the Camp Fire. Google trends data showed higher search activity for "air quality" and "N95 masks" during the Camp Fire compared to the Mendocino Fire. Public health interventions (school closures, advisories to stay indoors and mask use) may have also reduced exposure.
However, they also propose an alternative explanation for the differences observed between the two fires: a phenomenon in the air pollution literature known as "depletion of the susceptibles." This effect occurs when individuals most at risk experience the outcome in response to the first high exposure, making them either ineligible or less likely to experience the outcome during subsequent high exposures.
Regardless, the study provides "some evidence," say the authors, that wildfire smoke can elevate cardiovascular risk, albeit with inconsistent effects across wildfires, and sets the stage for future research to better quantify the role of protective actions.
Long-Term Effects of Wildfire Smoke
Beyond the short-term effects of wildfire smoke on cardiovascular and respiratory illness, understanding the long-term, cumulative effects of wildfire smoke exposure is crucial. Ma, et al., conducted a nationwide retrospective cohort study that aimed to quantify the association between prolonged exposure to wildfire-related PM2.5 and mortality across various disease categories in the contiguous U.S. from 2007 to 2020.3
The study analyzed monthly PM2.5 exposure data across all 3,108 counties in the contiguous U.S. and linked it to nationwide mortality records. Statistical models controlled for nonwildfire PM2.5, air temperature, seasonality and geographic variations to isolate the effects of wildfire-specific pollution.
The results revealed that higher levels of wildfire PM2.5 were significantly associated with increased mortality from cardiovascular diseases, ischemic heart disease, diabetes, kidney disease, and mental disorders such as dementia and posttraumatic stress disorder.
Annually, wildfire smoke was estimated to contribute to more than 11,400 excess deaths across the contiguous U.S., with the greatest burden on cardiovascular diseases (4,512 deaths). Older adults and racial minorities, particularly Black and Hispanic populations, faced disproportionately higher risks.
"A unique feature of wildfire smoke is that it can travel for hundreds of miles, affecting air quality for millions of people far from the fire source, as these findings confirm. This makes wildfires not just a problem for regions prone to fires but a national and international public health issue," says Kai Chen, PhD, the senior author on the study and an environmental epidemiologist at the Yale School of Public Health. He focuses on the intersection of climate change, air pollution and human health and is an associate editor at JACC. (See sidebar.)
The study also found that extreme heat amplified the effects of wildfire smoke, significantly increasing mortality risks, particularly for cardiovascular and mental health outcomes.
Interestingly, the study found that compared to periods with very low smoke exposure (<0.1 μg/m3), mortality increased in different ways at different concentration levels:
- At lower concentrations (0.1-1 μg/m3), there were modest but significant increases in mortality
- At moderate concentrations (1-5 μg/m3), the effect appeared to level off somewhat
- At high concentrations (>5 μg/m3), there was a much larger jump in mortality risk, with death rates increasing by about 2.11 deaths per 100,000 people per month.
This nonlinear relationship highlights the need for more research into what factors might modify these effects, more sophisticated ways to assess health impacts that consider these varying levels of risk, and public health responses that consider both low-level chronic exposure and extreme exposure events, suggest the researchers.
Temperature Extremes and Heart Disease
Climate change has increased the frequency and intensity of heatwaves, which have been linked to elevated heart disease mortality. However, prior studies have mainly used binary definitions of heatwaves (heatwave vs. nonheatwave days), which fail to capture the potential nonlinear relationship between heatwave exposure and cardiac mortality.
In a recent JACC paper, Xue Yu, MD, and colleagues in China report a nationwide, individual-level, case-crossover study that used heart disease mortality records from mainland China (2013-2019) and employed a novel and continuous metric to classify heatwaves into daytime-only heatwaves (hot days, but not nights), nighttime-only heatwaves (hot nights, but not days), and compound heatwaves (hot days and nights combined).4
In studying nearly 2.4 million heart disease deaths (64% in individuals over 74 years and 79% occurring outside the hospital), the researchers found that different types of heatwaves had varying impacts on mortality. Compound heatwaves posed the greatest risk, nearly doubling the odds of death (an 86% increase). In comparison, heatwaves occurring only at night or only during the day had much lower risks, increasing the odds of mortality by 16% and 19% respectively.
The numbers tell a striking story: compound heatwaves were associated with 41,869 excess cardiac deaths, while nighttime-only heatwaves led to 9,092 excess deaths and daytime-only heatwaves to 9,809. Together, these represented about 2.5% of all heart disease deaths studied.
Importantly, these numbers are significantly higher than those obtained using traditional yes-no methods of measuring heatwaves. Additionally, different heart conditions displayed varying levels of vulnerability. Sudden cardiac arrest, myocardial infarction and heart failure were the most sensitive to compound heatwaves, while pulmonary heart disease showed the least impact.
"This study incorporated multiple characteristics of excess temperature to examine cumulative temperature exposure rather than using the traditional binary approach," explains Chen. The researchers found a significantly greater risk for cardiac mortality during excessively hot days and nights, information that is valuable for clinicians and public health agencies looking for the best ways to protect people from extreme heat events," he adds.
Looking at the impact of high temperatures on the burden of ischemic heart disease (IHD) in Asia over the last 30 years, there as been a significant increase, with the greatest impact on men, older populations and those living in South Asia.5 Using data from the Global Burden of Disease 2021 study, Qinyi Bao, MD, Jian'an Wang MD, PhD, FACC, et al., found that the age-standardized annual increase in IHD burden was 1.63% for mortality and 1.60% for disability-adjusted life years (DALYs) from 1990 to 2021. A total of 88,450 deaths and 2,11,025.42 DALYs were reported in 2021. The authors note that 2023 marked the 27th consecutive year of above-average temperatures in Asia.
The Domino Effect: When Disasters Multiply
Natural catastrophes and extreme weather events don't tend to happen in isolation. Compound events, such as the simultaneous or sequential occurrence of droughts or wildfires with heatwaves, have become more common, and their frequency is expected to continue to increase.
Understanding these compound risks requires considering the "exposome" – the totality of environmental exposures that impact human health throughout life. This framework helps explain how multiple climate-related stressors can interact and accumulate over time.
"Multiple climate-related stressors interact and work synergistically to amplify health risks, resulting in a much larger impact than if we studied each one individually," says Chen. "The severity of the recent LA wildfires, for example, is clearly related to the drought event that was happening before, adding more fuel to the fire and prolonging the wildfire season into winter."
During such compound events, a person's exposome might include simultaneous challenges: direct heat stress, increased air pollution from wildfires, changes in physical activity patterns, emotional stress, disrupted sleep and dehydration risks. These overlapping exposures can overwhelm both individual physiological resilience and health care system capacity. Research suggests the cardiovascular impacts of combined stressors may be greater than the sum of individual exposures.
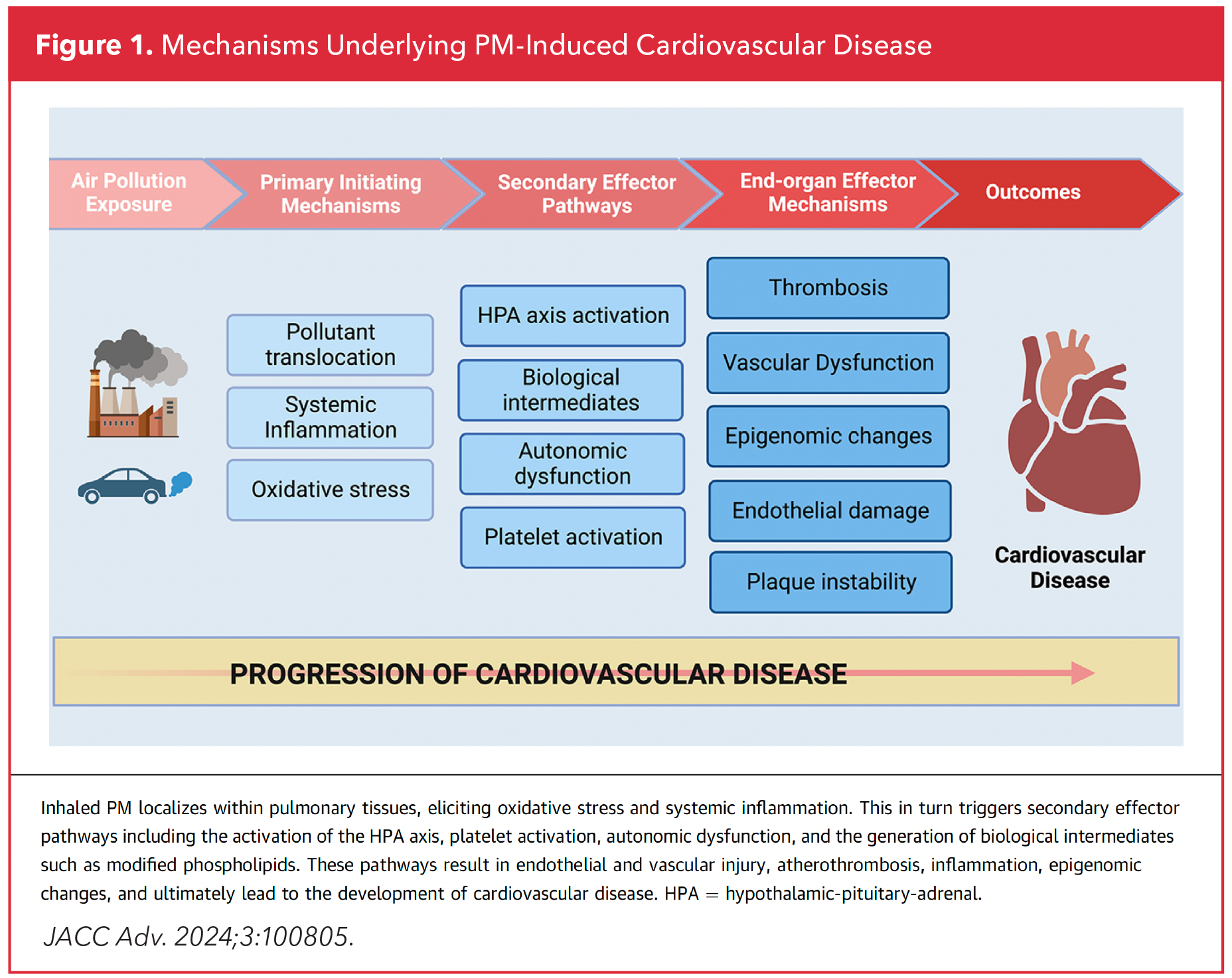
The mounting epidemiological and pathophysiological evidence links air pollution – both ozone and PM2.5 – to cardiovascular disease (Figure 1).6,7 This has spurred cardiologists to take decisive action, from creating patient education tools to advocating for broader systemic changes.
As Rana observes, "The recent apocalyptic wildfires in Los Angeles are yet another unfortunate reminder that climate change is an existential threat, and studying its relationship with cardiovascular disease is an imperative for the field of climate cardiology."
Beyond Survival: Strategies For Prevention and Adaptation
"Patients ask all the time, 'How did this happen? I'm healthy and active; how did I end up with heart disease?' In my response, I often include pollution as a contributor given all we know now about the link between pollution and increased cardiovascular events," says Colin T. Phillips, MD, FACC, an interventional cardiologist at MaineHealth Maine Medical Center in Portland, ME.
Phillips is the chair of the ACC Board of Governors Climate Change Work Group, a diverse group of cardiologists who convened in 2023 with the goal of bringing greater attention to the effects of climate change on cardiovascular health.
Says Phillips, "Over the last 30 years, the data have grown and become more impressive that, in fact, pollution hurts us. And it hurts us through numerous mechanisms. The end result is often cardiovascular events."
To help teach the basics on air pollution, its impact on the heart, and steps to take to lower risk, the Work Group collaborated with patients and ACC's CardioSmart to create an infographic for patients.
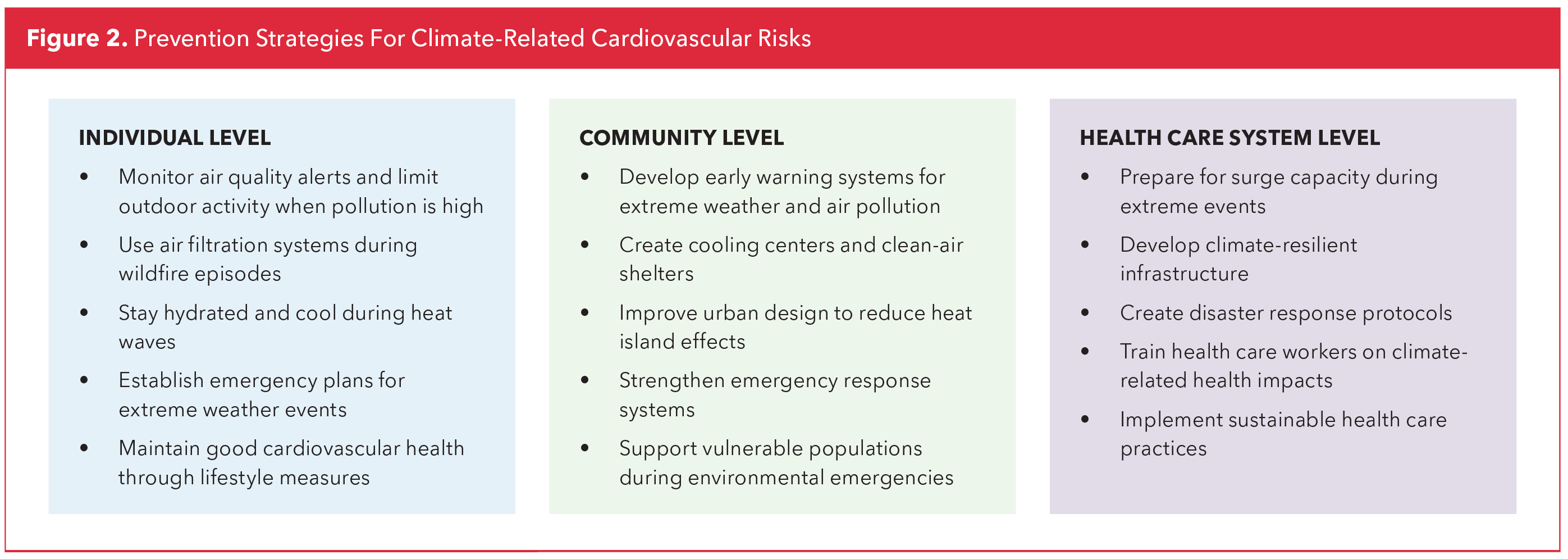
As climate-related health threats intensify, the focus must shift from reactive responses to proactive prevention and adaptation strategies. Recent research has identified several effective approaches for reducing cardiovascular risks during extreme weather events, with particular attention to vulnerable populations (Figure 2).
In terms of what patients should do when air quality is bad or temperatures are high, most agree on the use of N95 masks and air purifiers, as well as cooling stations. Also, people, and particularly those with respiratory and cardiac conditions, are advised to avoid exercising outside on bad air quality day. "I tell my patients, look, you wouldn't go outside for a run in a hurricane, don't go outside for a run when the air quality is bad," says Phillips.
Of note, a 2024 study from the University of Sydney and Montreal Heart Institute challenges some conventional wisdom about cooling strategies. The research found that simple interventions like electric fans and skin wetting can significantly reduce cardiac strain in older adults during extreme heat – but only under specific conditions. While these methods proved beneficial in hot, humid environments up to 100° F (38°C), fan use became dangerous in very hot, dry conditions above 113°F (45°C). Such nuanced findings highlight the importance of evidence-based guidance for public health recommendations.
"While we often assume staying indoors is safer than being outside during poor air quality events, the reality depends on ventilation and filtration. We need more research to understand when indoor air is actually better and how to optimize indoor spaces to protect health," notes Harlan Krumholz, MD, SM, FACC, from Yale University and editor-in-chief of JACC.
Health care systems are also adapting their approaches. This includes developing early warning systems for extreme weather events, creating protocols for surge capacity during disasters and implementing climate-resilient infrastructure. Special attention is being paid to protecting vulnerable populations, particularly those with preexisting cardiovascular conditions or limited access to air conditioning.
Community-level interventions have proven crucial. Cities are increasingly establishing cooling centers, improving urban design to reduce heat island effects and strengthening emergency response systems.
For individuals with cardiovascular disease, physicians are developing personalized adaptation strategies. These include adjusting medication schedules during extreme heat, providing specific guidance about indoor cooling methods, and creating emergency plans for power outages or evacuation scenarios. The goal is to build resilience at both individual and system levels, recognizing that climate adaptation must become a fundamental part of cardiovascular care.

Helping Patients Protect Their Hearts
Created by the Climate Change Work Group and CardioSmart, this infographic supports conversations with patients on the impact of air pollution on heart health and steps they can take to reduce the risk.
JACC Commits to Advancing Environmental CV Health Research
JACC has recognized the growing frequency and threats posed by extreme weather events and prioritized environmental health research, building a platform for groundbreaking studies and interdisciplinary dialogue that will shape our approach to this issue.
"We want to make it clear to the cardiology and broader scientific communities that environmental health is a critical frontier for cardiovascular research – one we must prioritize to protect patients," says Editor-in-Chief Krumholz.
To support this initiative, JACC has appointed Chen as an associate editor specializing in environmental health and assembled a global team of experts dedicated to investigating climate-driven cardiovascular risks. Recent JACC publications have explored the effects of air pollution, extreme heat and cold spells on heart disease, emphasizing the need for evidence-based interventions.
"We understand some acute cardiovascular effects of climate events, but we know far less about the long-term risks, repeated exposures, and – most importantly – how to mitigate these dangers," Krumholz adds.
Additionally, Krumholz is advocating for more and better data on how climate-related disruptions to health care systems affect cardiovascular outcomes and improved surveillance systems to capture real-time cardiovascular events during climate disasters.
Beyond publishing research, JACC is calling on the cardiovascular community to "lead the charge" in anticipating, mitigating and adapting to the realities of climate change. This should include enhancing public health surveillance to monitor cardiovascular risks during extreme weather and wildfire events, investing in climate-resilient health care infrastructure to protect vulnerable patients, including emergency power supplies, portable air filtration units and mobile health units, and proactive measures like stockpiling emergency medications and conducting post-disaster screenings to minimize secondary impacts.
"While climate change is a macro issue, cardiovascular specialists have long tackled public health challenges – just as we did with smoking. Ultimately, this is about changing behaviors to protect heart health, which is central to our mission," says Krumholz.
By leading the charge in environmental cardiovascular health research, JACC is ensuring that the cardiology community remains proactive in addressing one of the defining public health challenges of our time.
Read more about JACC's commitment to environmental cardiovascular health research and a call to action in an Editor's Page from Chen, Lu and Krumholz.
This article was authored by Debra L. Beck, MSc.
References
- Global Newswire. U.S. Air Purifier Market Share & Trends Analysis Report 2025-2030, with Key Players Daikin Industries, Honeywell International, LG Electronics, Panasonic Corporation and IQAir Group. Accessed March 13, 2025. Available here.
- Alexeeff SE, Van Den Eeden SK,. Wildfire air pollution and rates of cardiovascular events and mortality in northern california in 2018. J Am Heart Assoc. 2025;Feb 5: 2025:e036264. doi:10.1161/JAHA.124.036264.
- Ma Y, Zang E, Liu Y, et al. Long-term exposure to wildland fire smoke PM2.5 and mortality in the contiguous United States. Proc Natl Acad Sci U S A. 2024;121:e2403960121. doi:10.1073/pnas.2403960121.
- Yu X, Liu J, Yin P, et al. Nonlinear relation between excess temperature in heatwaves and cardiac mortality: Exposure response in 2.39 million patients. J Am Coll Cardiol. 2025:March 25: DOI: 10.1016/j.jacc.2025.01.034.
- Bao Q, Wang Z, Wang J, et al. Epidemiology of ischemic heart disease burden attributable to high temperature in Asia from GBD 2021. JACC: Asia. 2025;Feb. 25: doi:10.1016/j.jacasi.2024.12.012
- Hua Q, Meng X, Chen W, et al. Associations of short-term ozone exposure with hypoxia and arterial stiffness. J Am Coll Cardiol. 2025;85:606-21.
- Sagheer U, Al-Kindi S, Abohashem S, et al. Environmental pollution and cardiovascular disease: Part 1 of 2: air pollution. JACC Adv. 2024;3:100805.
Clinical Topics: Cardiovascular Care Team
Keywords: Cardiology Magazine, ACC Publications, Extreme Weather, Air Pollution, Climate Change, Wildfires, Public Health