Earlier Ablation For AFib Associated With Improved CV Outcomes
Atrial fibrillation catheter ablation (AFCA) improved clinical outcomes compared with medical treatment alone, and early AFCA was associated with better outcomes than late AFCA, particularly decreased risk of heart failure (HF) hospitalization and atrial fibrillation (AFib) recurrence, according to a new retrospective study published Feb. 19 in JACC: Clinical Electrophysiology.
In a nationwide cohort study, Soonil Kwon, MD, et al., investigated a total of 57,804 patients (mean age 57.8 years; 73.5% men; mean CHA2DS2-VASc score 2.2; average follow-up of 2.6 years) with AFib using the Korean National Health Insurance Service claims database from 2009 to 2020. Patients were matched at a 2:1 ratio between those who did not receive AFCA (n=38,536) and those who did (n=19,268). Both arms had similar demographics.
Patients in the AFCA arm were then categorized based on how soon they had a first ablation after AFib diagnosis: early AFCA (less than one year after diagnosis, n=7,511), intermediate AFCA (one to three years, n=6,197) and late AFCA (more than three years; n=5,560). Radiofrequency catheter ablation was most commonly used in all three categories, but a higher proportion of patients underwent cryoablation in the late than the early AFCA arms (13.9% vs. 7.8%).
Results showed that compared with medical treatment alone, AFCA was associated with a lower risk of major adverse cardiovascular events (MACE, defined as ischemic stroke, HF hospitalization, myocardial infarction [MI]) (hazard ratio [HR], 0.29; 95% CI, 0.26-0.32; p<0.001). This was also seen for the individual components of the endpoint: ischemic stroke (HR, 0.27), HF hospitalization (HR, 0.29) and MI (HR, 0.41), as well as all-cause mortality (HR, 0.26) and a composite outcome including all these events (HR, 0.27); p<0.001 for all.
Among the AFCA cohort, the risk for HF hospitalization and all-cause mortality was higher in the intermediate and late, vs. early, AFCA groups. Late AFCA was associated with a higher risk of MACE, composite outcomes and AFib recurrence compared with the other groups.
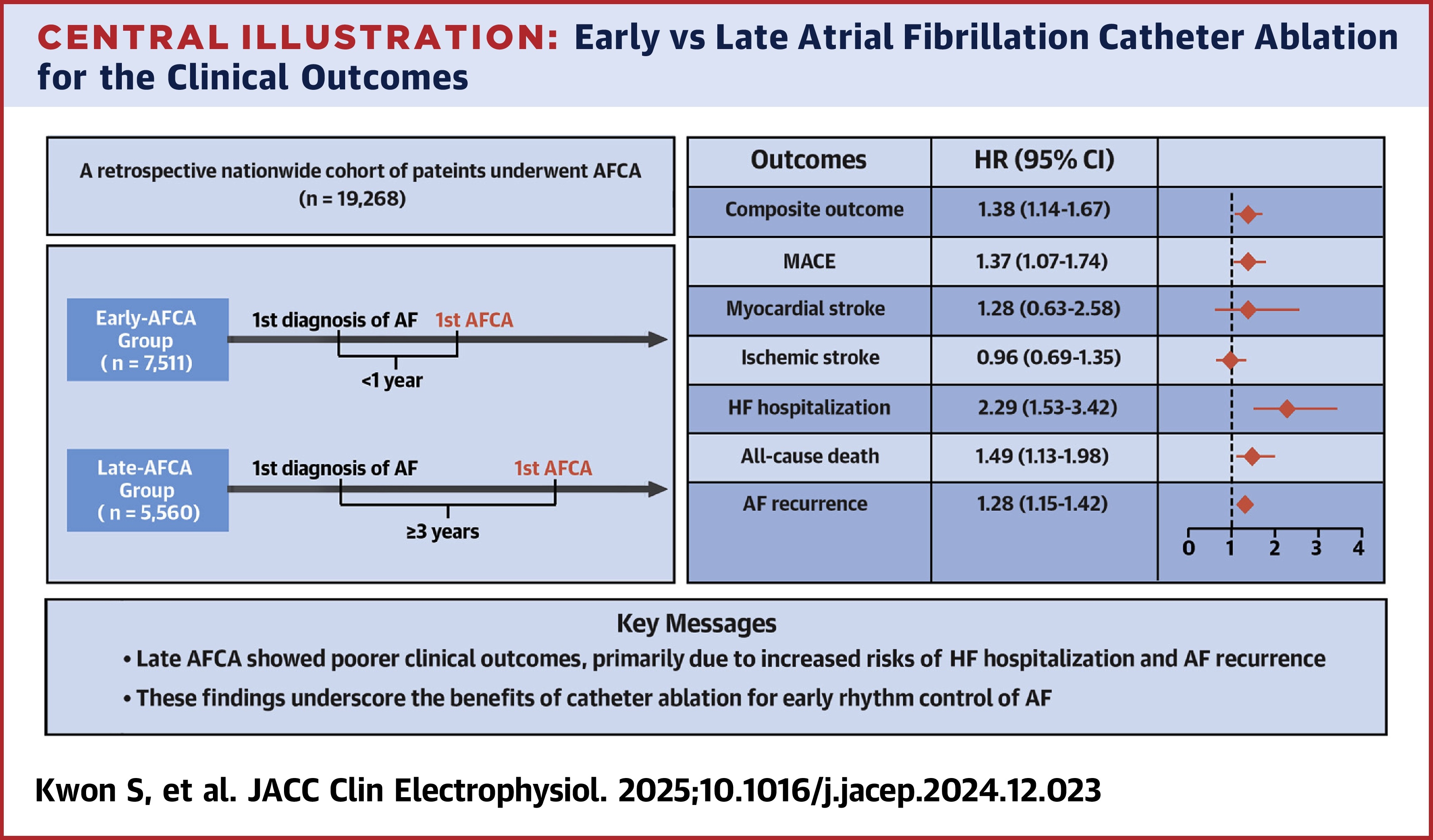
Compared with early AFCA, a delay of more than three years increased the risk of MACE by 37%, HF hospitalization by 129%, all-cause mortality by 49% and AFib recurrence by 28%.
"The efficacy of AFCA might decrease if delayed because as AFib progresses, pathophysiological changes lead to the involvement of nonpulmonary vein triggers and atrial cardiomyopathy, which contribute to the development of persistent AFib," write the authors. "Therefore, early AFCA could potentially prevent AFib progression and result in lower recurrence rates than medical treatments alone."
Clinical Topics: Arrhythmias and Clinical EP, SCD/Ventricular Arrhythmias, Atrial Fibrillation/Supraventricular Arrhythmias
Keywords: Catheter Ablation, Atrial Fibrillation
< Back to Listings