Impact of HFpEF on Ablation Outcomes; PVI Only Ablation in HFrEF?
Patients who undergo catheter ablation for atrial fibrillation (AFib) who also have heart failure with preserved ejection fraction (HFpEF) experienced a greater benefit from ablation in terms of clinical outcome, AFib recurrence and functional status, according to findings from the CABANA trial published April 16 in JACC: Heart Failure. Another recent retrospective study in patients with heart failure and reduced ejection faction (HFrEF) published in JACC: Clinical Electrophysiology found that adding line/low-voltage ablation (L/LVA) on top of pulmonary vein isolation (PVI) increases the risk of overall and nonvascular complications while the benefit is unclear.
The post hoc analysis from CABANA included the 1,763 patients whose H2FPEF score could be calculated; 55% had a score ≥6. Per enrollment criteria, all had at least one cardiovascular risk factor for stroke and either two or more episodes of paroxysmal AFib or one episode of persistent AFib in the previous six months.
These patients tended to be older, more often White, with a higher BMI and blood pressure level; they more often had diabetes, coronary artery disease and obstructive sleep apnea and worse functional status. The median LVEF was 59%.
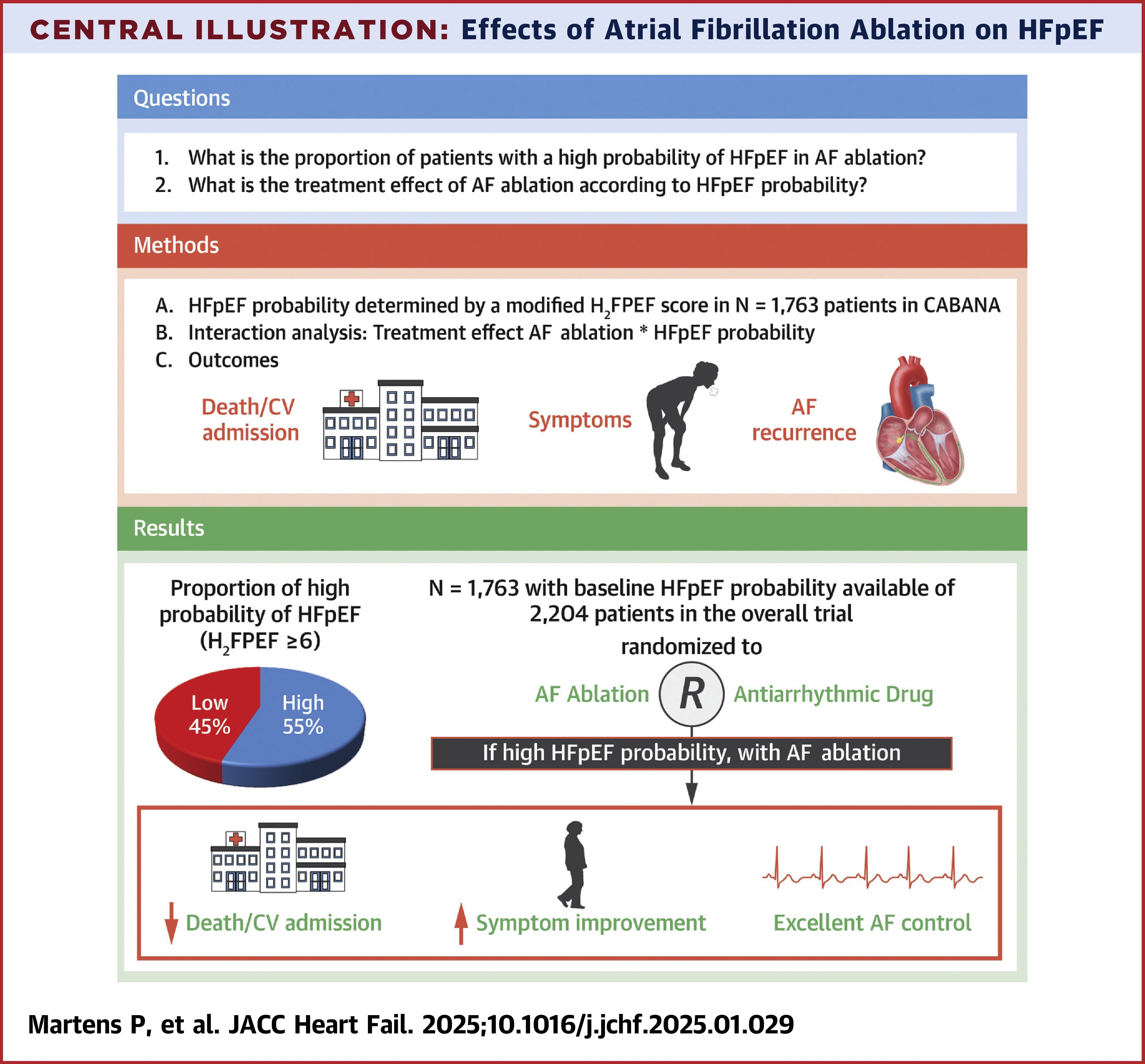
Results showed that a modified H2FPEF score of ≥6 was associated with a significant treatment effect (pint=0.027) with a lower risk of cardiovascular hospitalization or death (hazard rate [HR], 0.82; p=0.025), but this was not observed in patients with lower scores. Also, a higher score was associated with a greater treatment effect of ablation on AFib recurrence (pint=0.035). Similar treatment effects were found in a sensitivity analysis using echocardiography to determine HFpEF instead of the H2FPEF score.
Noting that the decrease in cardiovascular admissions seemed to drive the reduction in the combined endpoint, Pieter Martens, MD, MSc, PhD; W.H. Wilson Tang, MD, FACC, et al, write, "This finding suggests that [AFib] ablation alters the clinical course in patients with HFpEF." They further note this observation is in line with the previous data showing that [AFib] ablation can lower pulmonary capillary wedge pressure in patients with HFpEF.
The retrospective observational study conducted in Europe and led by Marco Bergonti, MD, PhD; Giulio Conte, MD, PhD, et al., included 955 patients with HFrEF who had undergone AFib ablation; 52% had only PVI ablation and 48% had PVI+L/LVA ablation. Overall, their mean age was 62 years and 25% were women.
At 12 months, for the two co-primary endpoints, 62% of patients were free of AFib recurrence and 65% had full recovery of ventricular function.
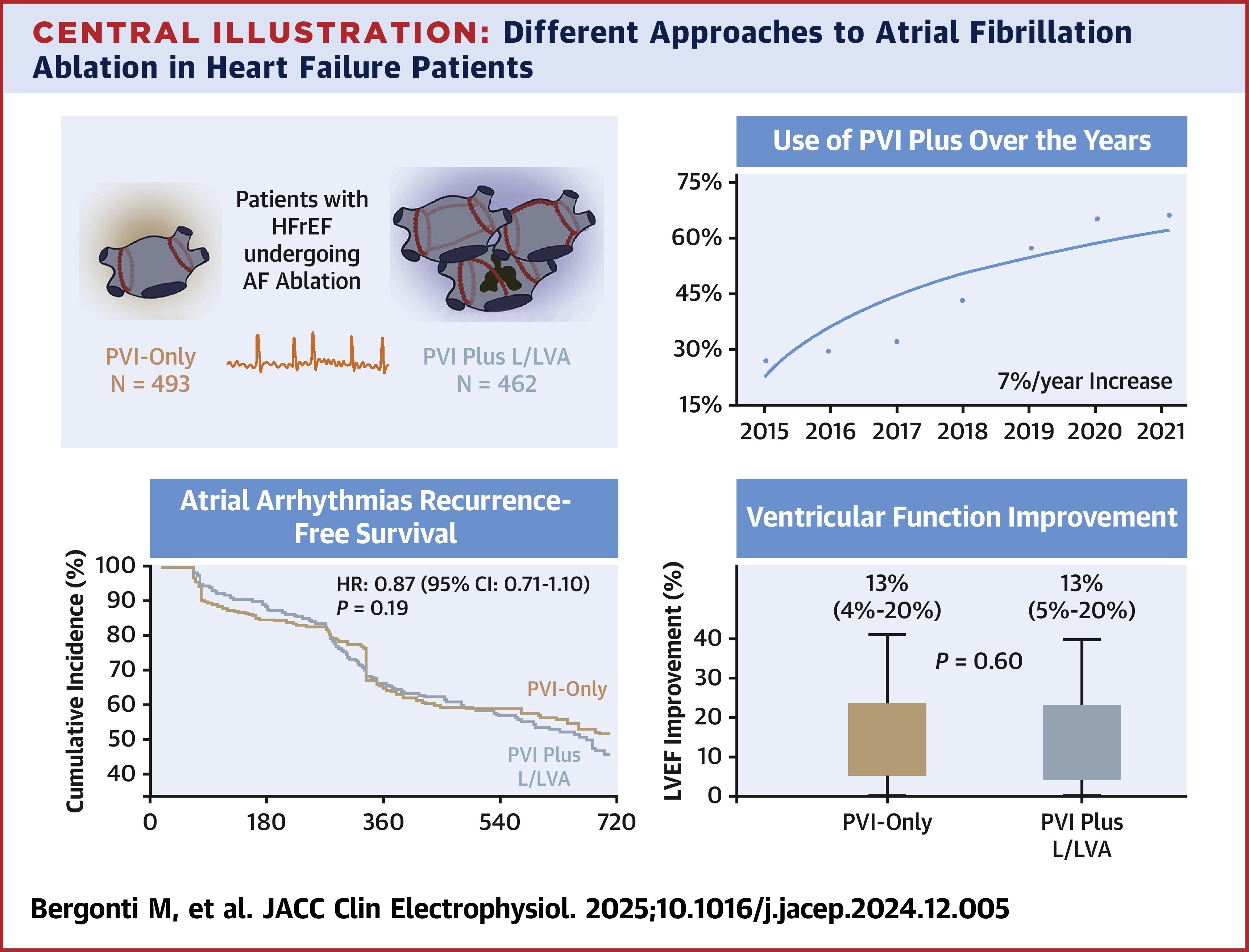
When comparing PVI and PVI+L/LVA between the overall cohort vs. two matched cohorts, no differences were observed in these outcomes. Freedom from AFib recurrence was 37% with PVI and 38% with PVI+L/LVA in the overall cohort vs. 31% and 36%, respectively, in the matched cohort. For LVEF recovery, the rates were 62% with PVI and 64% with PVI+L/LVA in the overall cohort and 68% with PVI and 71% with PVI+L/LVA in the matched cohort.
Procedural complications occurred more frequently with PVI+L/LVA than with PVI (3.7% vs. 1.2%).
"Our study does not support the concept that no additional ablation set on top of PVI is beneficial but advises caution against the rapidly increasing use of PVI+L/LVA in unselected patients with HFrEF, especially in light of the increased complication rate," write the authors.
"In many studies on ablation of persistent [AFib], the majority of patients (around 65%) had normal atrial tissue and were as successfully treated with a PVI-alone approach as paroxysmal patients," write Vanessa Sciacca, MD, and Philipp Sommer, MD, in an accompanying editorial comment. "Therefore, a generalized 'PVI+' strategy might lead to overtreatment of a relevant proportion of patients and may increase the rate of atrial tachycardia recurrences because of incomplete lesions in healthy atrial tissue."
Citations:
- Martens, P, Augusto, S, Erzeel, J. et al. Effects of Atrial Fibrillation Ablation for Heart Failure With Preserved Ejection Fraction: Insights From CABANA. J Am Coll Cardiol HF. Published online April 16, 2025. doi: j.jchf.2025.01.029
- Bergonti, M, Krisai, P, Ascione, C. et al. Different Approaches to Atrial Fibrillation Ablation in Heart Failure Patients: Temporal Trends and Clinical Outcomes. J Am Coll Cardiol EP. Published online April 16, 2025. doi: 10.1016/j.jacep.2024.12.004
Clinical Topics: Arrhythmias and Clinical EP, Heart Failure and Cardiomyopathies, Atrial Fibrillation/Supraventricular Arrhythmias, Acute Heart Failure
Keywords: Pulmonary Veins, Atrial Fibrillation, Heart Failure
< Back to Listings