Focus on Heart Failure | Beyond Steroidal MRAs: Rethinking MR Blockade in HF

Mineralocorticoid receptor antagonists (MRAs) are foundational in heart failure with reduced ejection fraction (HFrEF).1,2 In patients with preserved or mildly reduced ejection fraction (HFpEF/HFmrEF), however, the evidence has been inconsistent and does not build a compelling case for the use of steroidal MRAs in HFpEF/HFmrEF. The TOPCAT trial was neutral overall, though the Americas subgroup suggested potential benefit with spironolactone.3 More recently, SPIRIT-HF, presented at ACC.26, did not demonstrate a benefit for spironolactone in HFpEF/HFmrEF; however, the trial was limited by enrollment disruptions from the COVID-19 pandemic, with over half of patients discontinuing study drug.4 Taken together, and acknowledging the limitations of both trials, the available evidence does not build a compelling case for the use of steroidal MRAs in HFpEF/HFmrEF.
Enter Finerenone
Finerenone is a nonsteroidal MRA with selective receptor binding, distinct co-regulator interactions and balanced heart-kidney distribution – properties that together produce a more targeted transcriptional profile than conventional steroidal MRAs.
In practice, this translates to fewer off-target hormonal effects, a more favorable tolerability profile and lower observed rates of hyperkalemia compared with steroidal MRAs.5,6
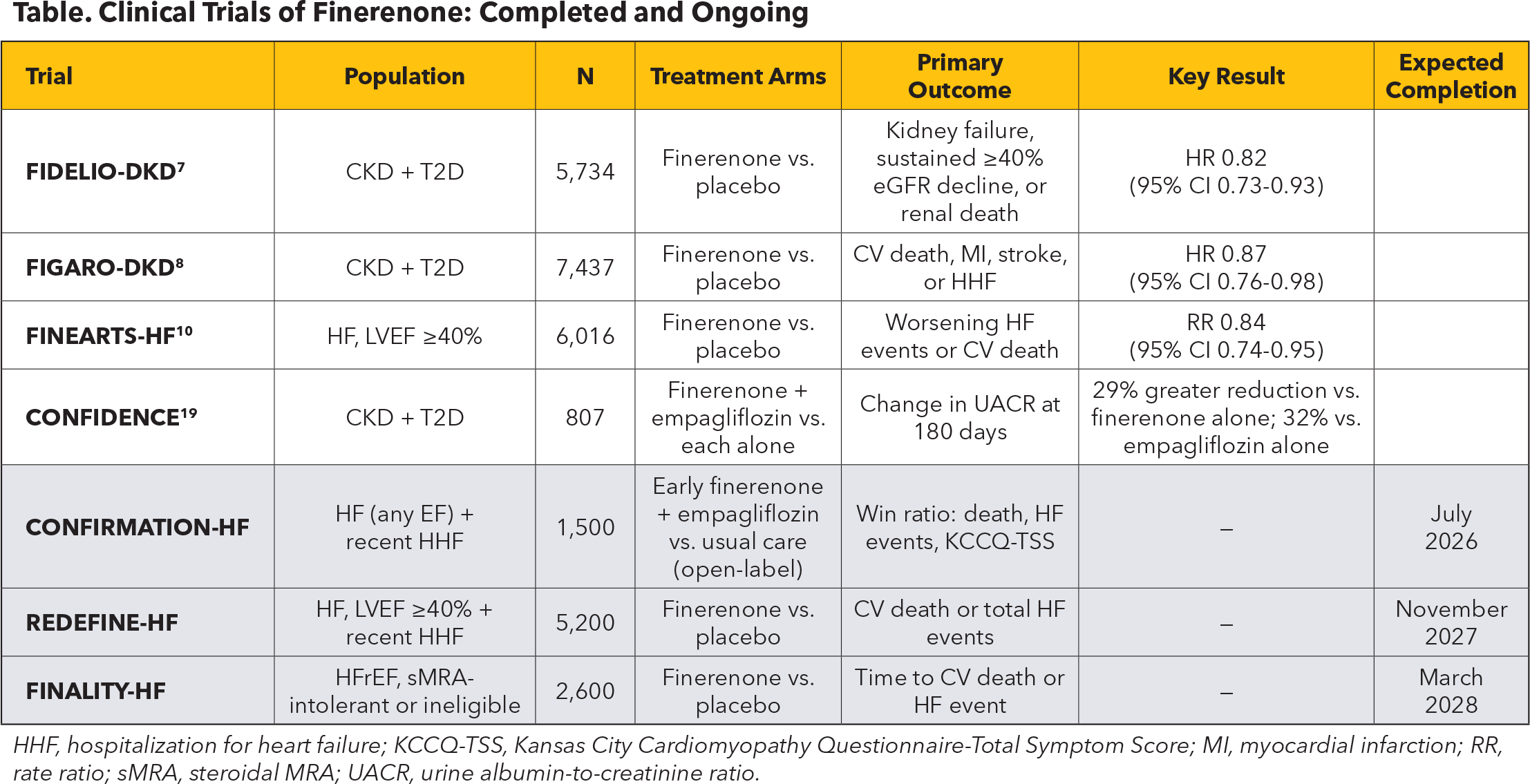
Its clinical development has followed a distinctive path in the cardio-kidney-metabolic space, with regulatory approval for chronic kidney disease (CKD) with type 2 diabetes (T2D) first – on the basis of FIDELIO-DKD, FIGARO-DKD and the FIDELITY pooled analysis7-9 – followed by expansion into HF. In FINEARTS-HF, finerenone reduced a composite of worsening HF events and cardiovascular death by 16% across 6,016 patients with HF and LVEF ≥40% (rate ratio, 0.84; 95% CI, 0.74-0.95; p=0.007),10 supporting U.S. Food and Drug Administration approval for HFpEF/HFmrEF in July 2025.
Safety in Clinical Practice: The eGFR Dip and Hyperkalemia
Two factors may contribute to early discontinuation of finerenone, as with other guideline-directed medical therapies: an early decline in estimated glomerular filtration rate (eGFR) and hyperkalemia.
The eGFR dip, approximately 2-3 mL/min/1.73 m2 within the first month, appears to be hemodynamic and reversible. A prespecified FINEARTS-HF analysis demonstrated that this decline does not portend worse cardiovascular outcomes, in contrast to spontaneous eGFR decline in the placebo arm.11 Consistently, in the FIDELITY pooled analysis, clinical benefits were preserved irrespective of early eGFR trajectory.12 These findings parallel other HF therapies and support tolerating modest creatinine increases without premature discontinuation of disease-modifying drugs.
Hyperkalemia remains a concern but appears manageable with routine monitoring. In FINEARTS-HF, potassium >5.5 mmol/L occurred in 14.3% of finerenone-treated patients vs. 6.9% with placebo; however, discontinuation due to hyperkalemia was infrequent (1.7% vs. 0.6%), and no fatal events were reported.13 For context, in the TOPCAT Americas cohort, potassium >5.5 mmol/L occurred in 25.2% of patients receiving spironolactone (vs. 8.9% with placebo). A target trial emulation in CKD further suggested lower hyperkalemia rates with finerenone compared with spironolactone (17.2% vs. 26.4%).14
Implementation and Future Directions
Despite a favorable efficacy-safety profile, implementation barriers remain. At approximately $700 per month – compared with approximately $10 for generic spironolactone – cost and prior authorization requirements may limit uptake. Real-world uptake of finerenone in CKD with T2D has already proven limited,15 echoing the well-documented therapeutic inertia seen across HF registries with other evidence-based therapies.16
The current ACC/AHA guideline for HF predates FINEARTS-HF,17 and guideline incorporation of finerenone – likely at Class IIa alongside SGLT2 inhibitors – is anticipated. Notably, FINEARTS-HF subanalyses have confirmed that the benefit of finerenone is preserved with concomitant SGLT2 inhibitor use in HF,18 while the CONFIDENCE trial demonstrated additive proteinuria reduction with the combination in patients with CKD and T2D.19 Together, these trials build the case for combination therapy across the cardio-kidney-metabolic spectrum.
The ongoing CONFIRMATION-HF trial, which is evaluating early initiation of finerenone plus empagliflozin vs. usual care after a HF hospitalization, will further inform the strategy of combining nonsteroidal MRAs with SGLT2 inhibitors.
Additional trials testing finerenone in HF are underway. Of particular interest is FINALITY-HF, evaluating finerenone in patients with HFrEF intolerant to steroidal MRAs – potentially filling a gap in real-world practice where hyperkalemia concerns limit uptake of an otherwise effective drug class.
Key Takeaways
Finerenone is the first MRA to demonstrate clear benefit in a pivotal trial in HFpEF/HFmrEF. Its safety profile positions it as a meaningful addition to the treatment algorithm and may extend to HFrEF patients unable to tolerate steroidal MRAs pending further trial data. Realizing this potential, however, will require overcoming the therapeutic inertia that has delayed the adoption of every major advance in HF pharmacotherapy.

This article was authored by Alberto Pinsino, MD, Cardiovascular Disease Fellow, New York Presbyterian Hospital, Columbia University Irving Medical Center, New York, NY.
References
- Pitt B, Zannad F, Remme WJ, et al. The effect of spironolactone on morbidity and mortality in patients with severe heart failure (RALES). N Engl J Med. 1999;341:709-717.
- Zannad F, McMurray JJV, Krum H, et al. Eplerenone in patients with systolic heart failure and mild symptoms (EMPHASIS-HF). N Engl J Med. 2011;364:11-21.
- Pfeffer MA, Claggett B, Assmann SF, et al. Regional variation in patients and outcomes in the Treatment of Preserved Cardiac Function Heart Failure with an Aldosterone Antagonist (TOPCAT) trial. Circulation. 2015;131:34-42.
- Edelmann F. SPIRIT-HF: spironolactone in heart failure with preserved or mildly reduced ejection fraction. Late-Breaking Clinical Trial, American College of Cardiology Scientific Session 2026; March 29, 2026; New Orleans, LA.
- Pandey AK, Bhatt DL, Cosentino F, et al. Non-steroidal mineralocorticoid receptor antagonists in cardiorenal disease. Eur Heart J. 2022;43(31):2931-2945.
- Harrington JL, Canonico ME, El Rafei A, et al. Nonsteroidal and steroidal mineralocorticoid antagonists: rationale, evidence, and unanswered questions. JACC Heart Fail. 2025;13(10):102637.
- Bakris GL, Agarwal R, Anker SD, et al. Effect of finerenone on chronic kidney disease outcomes in type 2 diabetes (FIDELIO-DKD). N Engl J Med. 2020;383:2219-2229.
- Pitt B, Filippatos G, Agarwal R, et al. Cardiovascular events with finerenone in kidney disease and type 2 diabetes (FIGARO-DKD). N Engl J Med. 2021;385:2252-2263.
- Agarwal R, Filippatos G, Pitt B, et al. Cardiovascular and kidney outcomes with finerenone in patients with type 2 diabetes and chronic kidney disease: the FIDELITY pooled analysis. Eur Heart J. 2022;43:474-484.
- Solomon SD, McMurray JJV, Vaduganathan M, et al. Finerenone in heart failure with mildly reduced or preserved ejection fraction (FINEARTS-HF). N Engl J Med. 2024;391:1616-1626.
- Matsumoto S, Henderson AD, Claggett BL, et al. Initial decline in glomerular filtration rate with finerenone in HFmrEF/HFpEF: a prespecified analysis of FINEARTS-HF. J Am Coll Cardiol. 2025;85:173-185.
- Navaneethan SD, Anker SD, Filippatos G, et al. Efficacy and safety of finerenone in patients with an acute change in estimated glomerular filtration rate in the prespecified FIDELITY pool analysis. Kidney Int. 2025;108(1):136-144.
- Rossignol P, Vaduganathan M, Engel LE, et al. Potassium changes with finerenone in heart failure with mildly reduced or preserved ejection fraction: a prespecified analysis of FINEARTS-HF. JAMA Cardiol. 2025;10(1):42-48.
- Wang CA, Lai H-W, Chen J-Y, et al. Finerenone versus spironolactone in patients with chronic kidney disease and type 2 diabetes: a target trial emulation. Nat Commun. 2025;16:9641.
- Lin W, Schweber A, Xu Y, et al. Finerenone utilization for chronic kidney disease and diabetes: multicenter real-world study in the United States. JACC Adv. 2026;5(4):102642.
- Greene SJ, Fonarow GC, DeVore AD, et al. Titration of medical therapy for heart failure with reduced ejection fraction. J Am Coll Cardiol. 2019;73:2365-2383.
- Heidenreich PA, Bozkurt B, Aguilar D, et al. 2022 AHA/ACC/HFSA guideline for the management of heart failure. J Am Coll Cardiol. 2022;79(17):e263-e421.
- Vaduganathan M, Claggett BL, Kulac IJ, et al. Effects of the nonsteroidal MRA finerenone with and without concomitant SGLT2 inhibitor use in heart failure: a prespecified analysis of FINEARTS-HF. Circulation. 2025;151(2):149-158.
- Agarwal R, Green JB, Mottl AK, et al. Finerenone with empagliflozin in chronic kidney disease and type 2 diabetes (CONFIDENCE). N Engl J Med. 2025;393:533-543.
Clinical Topics: Cardiovascular Care Team, Heart Failure and Cardiomyopathies, Acute Heart Failure
Keywords: Cardiology Magazine, ACC Publications, CM-Jun-2026, Heart Failure, Preserved Ejection Fraction, Hyperkalemia, Heart Failure, Reduced Ejection Fraction, Mineralocorticoid Receptor Antagonists, Heart Failure