Cover Story | Renal Denervation: Expanding Care For Treatment-Resistant Hypertension

Hypertension remains the leading global cause of death and disability, with more than half of hypertensive individuals in the U.S. failing to meet guideline-directed blood pressure (BP) targets. This scenario underscores a significant public health challenge driven by factors such as patient nonadherence, physician inertia and complex polypharmacy regimens. Against this backdrop, catheter-based renal denervation (RDN) has emerged as a novel interventional strategy for the management of treatment-resistant hypertension.
RDN involves the selective disruption of the sympathetic nerves located in the renal arteries. By ablating these nerves, RDN aims to reduce sympathetic activity, thereby lowering BP. The procedure is performed using various methods, including radiofrequency ablation, ultrasound or perivascular injection of neurotoxic agents.
The journey of RDN in clinical practice has been a bumpy one, marked by both great enthusiasm and real skepticism. Initial trials were promising, but then the sham-controlled SYMPLICITY HTN-3 trial, published in 2014, showed no significant BP reduction compared with sham procedures, raising questions about the efficacy of the strategy.1
The negative result seen in SYMPLICITY HTN-3 was ultimately attributed to a number of design and methodological limitations, including suboptimal and incomplete denervation in some patients, questionable medication adherence, high rates of drug changes during the trial, and variability in BP measurement technique across sites.
After SYMPLICTY HTN-3, trials of RDN slowed considerably, but over time clinical consensus conferences in Europe and the U.S. reassessed the findings and made recommendations regarding optimized technique, ensuring complete circumferential ablation of renal nerves, along with strict criteria for patient inclusion and objective measures of medication adherence.
In an interview with Cardiology, interventional cardiologist and key RDN researcher David E. Kandzari, MD, FACC, shares how things have changed in the RDN trial world. "Now, in all contemporary trials of RDN, we rely on ambulatory blood pressure monitoring, which is more reliable than office blood pressure measures. We test blood and urine samples for evidence of adherence, and we ensure there is a sham control and proper technique for ablation." Kandzari is chief of the Piedmont Heart Institute and Cardiovascular Services and chief scientific officer for Piedmont Healthcare in Atlanta, GA.
Subsequent studies with improved trial designs, including SPYRAL HTN-OFF MED, SPYRAL HTN-ON MED and RADIANCE-HTN SOLO, have demonstrated significant and consistent BP reductions in both ambulatory and office settings (Figure 1).
"We now have 13 sham-controlled, randomized clinical trials with RDN – nine with the two technologies approved by the U.S. Food and Drug Administration (FDA) and four others with investigational devices – that all demonstrate consistent safety and efficacy with meaningful reductions in BP that are sustained over follow-up (Figure 2)," reports Kandzari.

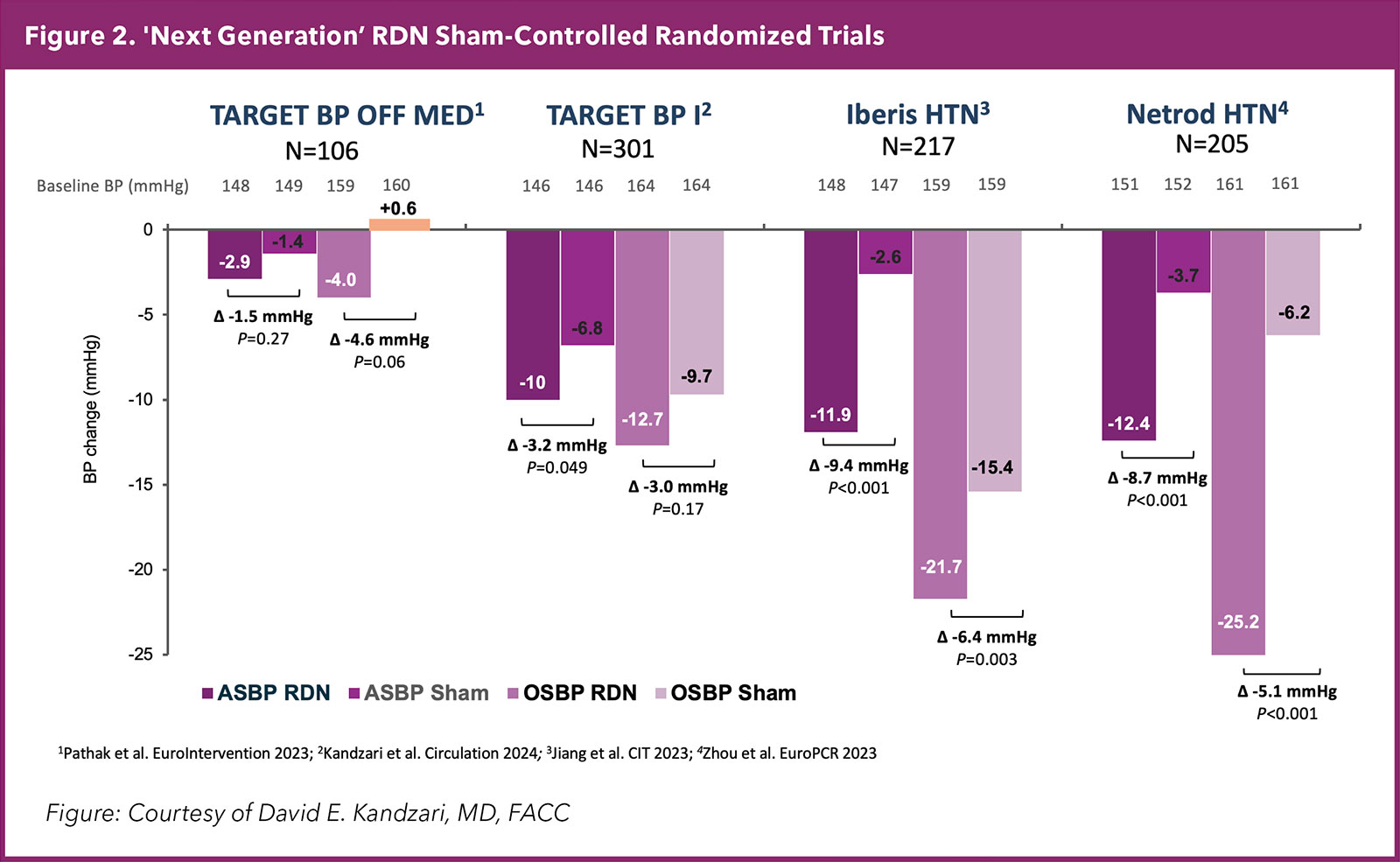
These trials highlight the potential of RDN as a viable therapeutic option for patients with treatment-resistant hypertension, he adds, and, notably, demonstrate efficacy in reducing BP independently of antihypertensive medications, addressing issues related to patient adherence and drug-related side effects.
Importantly, RDN has been shown to have an "always on" effect, lowering BP consistently over a 24-hour period. "This is especially relevant for individuals whose BP phenotype conveys a particularly high risk of adverse events, like stroke and death, such as individuals who have nocturnal or early morning hypertension," says Kandzari.
– David E. Kandzari, MD, FACC
Much of the data on RDN comes from Europe. In 2010, the Medtronic Symplicity Spyral device was the first to receive a CE mark. Since then, several other devices also have been approved. Medtronic's post-approval registry, called the Global Symplicity Registry (GSR), now offers up to three -year data on more than 3,000 patients. "The GSR data show real-world outcomes both in terms of effectiveness and safety that are consistent with what has been shown in the clinical trials," says nephrologist Debbie Cohen, MD.
"From the data, randomized and otherwise, RDN appears to offer a consistent reduction in BP of around 10 mm Hg systolic," says Cohen, director of the Hypertension Programs at Penn Medicine in Philadelphia, PA.
Overall, in 36 months of follow-up in the GSR, the office and 24-hour systolic BP reductions from baseline were −16.7 and −9.1 mm Hg, respectively (p<.0001).2 These reductions were independent of the number and type of baseline antihypertensive medication classes.
What's also been consistent across studies, adds Cohen, is that about one-quarter of patients do not respond to RDN. Identifying predictors of response remains a challenge.
"The only reliable predictor of response we've seen so far is that those with higher baseline BP have greater BP reductions," says Cohen. While enrollment in clinical trials requires appropriate evaluation to rule out secondary causes of hypertension, she suspects at least some of the patients defined as having resistant hypertension who are unresponsive to RDN in fact have undiagnosed primary aldosteronism. "These patients are not going to respond to RDN because the pathophysiology of their hypertension is different."
Primary aldosteronism is one of the more common causes of secondary hypertension, along with renovascular disease. Depending on the population screened, the prevalence ranges from 3.2% to 12.7% in primary practice and from 1% to 30% in referral centers.3 Prevalence increases with the severity of hypertension to 20%.3
"What we can tell patients at this point, based on data from three years of research, is that they may experience a reduction of around 17-20 mm Hg in systolic BP. Most of this reduction is incremental with a gradual decrease in BP over time," explains Cohen.
"This degree of BP reduction is clinically significant in terms of reducing the risk of cardiovascular events and in some patients may be sufficient to reduce their medication intake," she adds.
Approved But Awaiting Reimbursement
ACC's free online course, Overcoming Challenges in Hypertension Management, is self-paced learning to equip clinicians with best practices to improve patient care. Click here to get started.
Acknowledging this trove of promising data, two RDN systems received FDA approval in the U.S. in November 2023: the Symplicity Spyral Renal Denervation System (Medtronic) and the Paradise Ultrasound Renal Denervation System (Recor Medical).
The Symplicity Spyral catheter uses radiofrequency energy to thermally ablate the renal sympathetic nerves. The Paradise catheter system uses ultrasound energy to achieve similar results. Both devices are labeled as adjunctive treatments to medications and lifestyle for patients needing BP lowering.
Reimbursement for RDN in the U.S. is currently variable and dependent on individual insurance policies and payer decisions. This is par for the course for an emerging therapy, but it is significantly limiting the numbers of patients who can receive the procedure.
"The biggest challenge and the greatest hindrance to utilization of RDN at this point is not patient demand or physician interest, but the economics of it. Absent wide reimbursement, we currently don't have an easy path to financially supporting the procedure," says Eric A. Secemsky, MD, MSc, FACC.
Secemsky is the director of vascular intervention at Beth Israel Deaconess Medical Center (BIDMC), and section head of Interventional Cardiology and Vascular Research at the Smith Center for Outcomes Research in Cardiology, all in Boston, MA.
– Eric A. Secemsky, MD, MSc, FACC
Currently, there are no national or local coverage determinations (NCDs/LCDs) for RDN. Medicare covers FDA-approved therapies that are deemed necessary and reasonable, but without an NCD, prior authorization is usually necessary.
Medicare Advantage plans must provide the same coverage as traditional Medicare, but in the absence of specific NCDs/LCDs, they may refer to commercial coverage policies. For private payers, coverage and prior authorization requirements vary greatly depending on the plan and insurer. New therapies like RDN may not be explicitly included or excluded in policies.
RDN procedures are described by Category III CPT codes, which are contractor priced, meaning each Medicare contractor sets their reimbursement rates. Because Category III CPT codes are used to collect usage data on emerging technologies and services, they do not generally have payment rates or relative value units assigned.
"Until we have a national coverage decision and dedicated reimbursement for the procedure, we are left with the challenge of providing this breakthrough technology to our at-need patients," explain Secemsky.
At BIDMC, Secemsky and his team have a staff member dedicated to pursuing insurance coverage for patients deemed appropriate for the procedure. "Thus far, with support from our reimbursement team, we have been successful in getting approval for the procedure, but it does require some coordinated effort."
With all that, Secemsky and team are enthused by their early cases. "We're doing both commercial and trial patients, and growing the program over time," he says. The reimbursement landscape is evolving, he adds, and hopefully permanent reimbursement will come in the near future.
How RDN Works to Lower BP
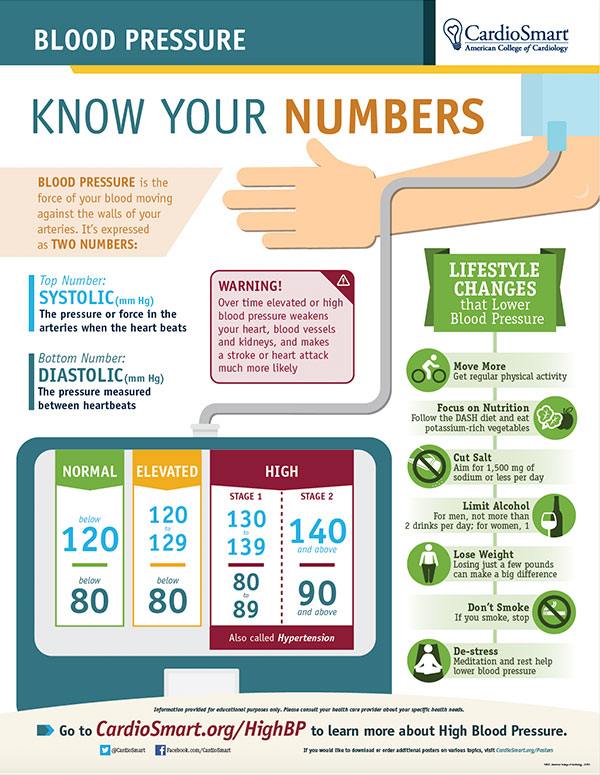
Patient Education
BP management is teamwork and infographics and tools for patients help support them in this partnership. Click here to download this infographic and explore more tools.
The sympathetic nervous system plays a significant role in the pathophysiology of hypertension, especially in patients with obesity, obstructive sleep apnea and chronic kidney disease. In many patients with hypertension, there is overactivity of the sympathetic nervous system, particularly the renal sympathetic nerves that run along the walls of the renal arteries.
These nerves carry signals from the brain to the kidneys (efferent) and from the kidneys to the brain (afferent). Efferent signals can increase renin release, sodium retention and renal vasoconstriction, all of which raise BP. Afferent nerves signal the central sympathetic activity leading to reflex sympathetic activation, peripheral vasoconstriction, increased BP and hypertension-mediated organ damage.
RDN selectively ablates or disrupts these renal nerves, reducing both whole-body and renal sympathetic activity. By reducing renal sympathetic nerve activity, RDN can decrease renin release, reducing angiotensin II and aldosterone levels; increase sodium and water excretion; reduce renal vasoconstriction, increasing renal blood flow; and decrease central sympathetic activity, reducing overall vascular tone.
Based on currently available data, durability of BP reduction has been shown up to three years after RDN in both the SYMPLICITY HTN-3 and the SYPYRAL HTN-ON MED trial, with limited data out to five and 10 years also showing sustained BP reduction.
Studies suggest the antihypertensive effects of RDN may be durable, possibly due to permanent disruption of the renal nerves or resetting of central sympathetic tone. As well, RDN has shown potential benefits beyond BP control, such as improvements in sleep apnea, left ventricular hypertrophy and albuminuria, all of which are related to sympathetic overactivity.4
Based on available data, there also appears to be no risk of chronic damage to the kidneys or the renal arteries themselves, such as unanticipated trauma or a decline in kidney function.
"But going one step further and thinking about whether there might be any physiologic risk of reducing the hyper-sympathetic signature within the body, we have not seen any compromise in the homeostatic mechanisms of individuals treated with RDN," says Kandzari. "In other words, there's no impact on the fight-or-flight response or the stressor response in an individual who, say, is losing blood and needs to quickly raise their BP, or is in septic shock such that their BP is too low."
What the Guidelines Say

"By my count, at least 18 societal and/or guideline consensus documents have now been published endorsing RDN as part of clinical practice, providing information with regard to patient selection for the therapy, and in some instances focusing on prioritizing certain patients for the treatment of RDN," offers Kandzari.
The inclusion of RDN as a therapeutic option in the latest European Society of Hypertension (ESH) Guidelines for the Management of Arterial Hypertension is perhaps the greatest endorsement of its growing acceptance based on accumulating evidence.3
The 2023 ESH guideline affords RDN a class II recommendation for patients with an eGFR >40 ml/min/1.73m2 who have uncontrolled BP despite the use of antihypertensive drug combination therapy, or if drug treatment elicits serious side effects and poor quality of life. A class II recommendation is also given for RDN as an additional treatment option in patients with true resistant hypertension (and eGFR is >40 ml/min/1.73m2).
"A class II recommendation is the highest level of recommendation they could apply in the absence of a clinical outcomes trial," says Kandzari. None of the nine completed sham-controlled, randomized clinical trials on the approved devices were large enough to be powered for hard endpoints, like mortality, he adds. Also, since in most trials, patients are allowed at a certain point to cross over to RDN, the numbers for comparison of hard outcomes are even smaller.
"But most important is that to do a trial of any medication or device like RDN with an estimated 3.5% risk over the long-term for major adverse cardiac events (death, stroke, myocardial infarction), a trial with a sample size of approximately 20,000 patients would be needed to show that kind of benefit, as we wrote in the European Society of Cardiology consensus document."4 It's unlikely such a trial will be done.
He does expect, however, that longer-term registries will start to show a benefit for RDN on hard outcomes, similar with studies that show benefit to BP lowering by other means.
"We don't have direct one-to-one studies showing a reduction in mortality with RDN, but keep in mind we don't have that with individual BP medicines either. When we talk about BP medicines improving survival, that's coming from large meta-analyses of multiple medicines."
Kandzari and Secemsky were first and senior author, respectively, of a 2021 expert consensus roundtable statement on RDN co-sponsored by the National Kidney Foundation and the Society for Cardiovascular Angiography and Interventions (SCAI).5 Their group provided a comprehensive look at the data on RDN and discussed at length the importance of patient-centered treatment decision-making for potential patients that might benefit.
That document was updated in 2023 in a SCAI Position Statement on RDN which addresses patient selection, reviews optimal procedural and technical considerations, proposes a roadmap for operator training and competency, and delineates institutional requirements for programmatic success.6 Secemsky and Kandzari also served as authors on this statement.
According to the SCAI statement, primary candidates for RDN are those with resistant hypertension (BP >130/80 mm Hg despite taking three or more antihypertensive medications, including a diuretic). Beyond that, patients with uncontrolled hypertension who have tried lifestyle modifications and medication but are intolerant to additional medications or do not wish to increase medication use can also be considered, after a shared decision-making process. Priority may also be given to patients with higher cardiovascular risk.
"I think what all health care providers taking care of people with hypertension are thinking about today is whether RDN is durable and safe – both in the short- and long-term – and whether it will lower BP for their patients as well as lower their risk of death or stroke or other adverse events," says Kandzari. He notes there are data to answer many of these questions and guidance from professional societies further supporting the use of this therapy.
Do Patients Prefer RDN?

One of the key lessons learned from the pre-approval trials of RDN is the importance of considering patient preference in therapy and addressing the issue of nonadherence. According to Kandzari, even when patients are informed that adherence is being monitored through blood and urine testing, a significant percentage, ranging from 40% to 60%, demonstrate either partial or complete nonadherence to medications.
Using nonadherence as an indicator of patient preference sends a clear message that patients are seeking alternatives to lifestyle interventions and medications, he adds.
Anna K. Krawisz, MD, a cardiologist and vascular medicine specialist at BIDMC works with Secemsky on patient recruitment for trials, shared decision-making and safety monitoring for RDN procedures.
She sees a diverse population of patients with resistant hypertension, often at advanced stages, or with refractory hypertension. "They bring with them a range of preferences, medication intolerances and comorbidities. I strive to help them understand the various treatment options available," Krawisz says.
She notes many patients are skeptical about the effectiveness of medications in controlling their BP because they have tried numerous medications over time and they have likely attempted lifestyle interventions with limited success. "Often they are open or even enthusiastic about the possibility of having a procedure that offers them long-term, continuous BP lowering." Others are flatly resistant to the idea of an interventional procedure.
Regardless, Krawisz emphasizes the importance of clearly explaining the limitations of RDN, including the possibility of no response to the treatment and the uncertainty surrounding its long-term effectiveness.
In the end, she finds there is seldom a single solution for patients with truly resistant hypertension. "We almost always need to use multiple modalities to get patients' BP under control. I'm happy to add RDN to the toolbox because I've seen a lot of patients really benefit from it."
More Studies, More Options
RDN is not the only therapeutic option changing the treatment landscape for hypertension. After years of drought, the field is now replete with new therapeutic options, including GLP-1 agonists for weight loss and the newly approved drug aprocitentan, an endothelin receptor antagonist for resistant hypertension.
Other potential therapeutic options being tested in trials include aldosterone synthase inhibitors (baxdrostat and lorundostat); an investigational subcutaneous single interference RNA agent, called zilebesiran, that inhibits angiotensinogen production; and a human monoclonal antibody with potent natriuretic peptide receptor-1 called XXB750.
"For 25 years we had nothing new to offer our patients and now we have several new options. It's an exciting time," says Cohen.
Moving forward, ongoing studies and registries will further clarify the role of RDN in managing hypertension and its impact on outcomes. As the field evolves, RDN has the potential to become a crucial tool in the fight against hypertension, offering hope to countless patients striving to control their BP.
This article was authored by Debra L. Beck, MSc.
References
- Bhatt DL, Kandzari DE, O'Neill WW, et al. A controlled trial of renal denervation for resistant hypertension. N Engl J Med 2014;370:1393-1401.
- Mahfoud F, Mancia G, Schmieder RE, et al. Outcomes following radiofrequency renal denervation according to antihypertensive medications: subgroup analysis of the global SYMPLICITY registry DEFINE. Hypertens 2023;80:1759-70.
- Mancia G, Kreutz R, Brunström M, et al. 2023 ESH Guidelines for the management of arterial hypertension The Task Force for the management of arterial hypertension of the European Society of Hypertension. J Hypertens 2023;41:1874-2071.
- Barbato E, Azizi M, Schmieder RE, et al. Renal denervation in the management of hypertension in adults. A clinical consensus statement of the ESC Council on Hypertension and the European Association of Percutaneous Cardiovascular Interventions (EAPCI). Eur Heart J 2023;44:1313-30.
- Swaminathan RV, East CA, Feldman DN, et al. SCAI position statement on renal denervation for hypertension: Patient selection, operator competence, training and techniques, and organizational recommendations. J Soc Cardiovasc Angiogr Interv 2023;2. Available here.
- Kandzari DE, Townsend RR, Bakris G, et al. Renal denervation in hypertension patients: Proceedings from an expert consensus roundtable cosponsored by SCAI and NKF. Catheter Cardiovasc Interv 2021;98:416-26.
Clinical Topics: Arrhythmias and Clinical EP, Cardiovascular Care Team, Prevention, SCD/Ventricular Arrhythmias, Atrial Fibrillation/Supraventricular Arrhythmias, Hypertension
Keywords: Cardiology Magazine, ACC Publications, Renal Artery, Denervation, Hypertension, Medication Adherence, Radiofrequency Ablation