Heart of Health Policy | 2026 Medicare PFS Final Rule; Ambulatory Specialty Model For HF

Dive Into the 2026 Medicare Physician Fee Schedule Final Rule
The Centers for Medicare and Medicaid Services (CMS) has released the 2026 Medicare Physician Fee Schedule (PFS) final rule, updating the PFS conversion factor from $32.3465 to $33.5675 for qualifying alternative payment model (APM) participants and $33.4009 for nonqualifying APM participants, increases of 3.77% and 3.26%, respectively. This duality is required by current law. These conversion factors include the 2.5% increase passed in the One Big Beautiful Bill Act. The rest of the conversion factor increase stems from policy changes that reduce payment for many services.
The overall reimbursement for cardiovascular services is projected to increase roughly 1% compared with 2025. Individuals and groups will see different impacts depending on patient populations and services offered. Due to other provisions discussed below, facility-based services for cardiology are projected to decline 7% while nonfacility services are projected to increase 5%.
Key proposals relevant to cardiovascular clinicians regarding payment policy are below.
- Efficiency Adjustment: The rule finalized an efficiency adjustment of –2.5% to the intra-service times and work relative value units (RVUs) of nearly all non–time-based codes in the PFS, citing efficiencies in performing medical services that accrue over time and are not captured in the normal process of developing the time and work RVUs. The adjustment represents a five-year lookback at the productivity adjustment derived from the Medicare Economic Index. CMS will calculate and apply the efficiency adjustment every three years moving forward. The agency has agreed to exempt any new CPT codes created and initially valued for 2026. This amendment only applies to brand new Category I CPT codes and does not exempt existing codes that were re-valued this year.
- Site of Service Payment Differential: A significant update to the payment methodology will change the way CMS pays for indirect practice expense (PE). Due to the rise of hospital employment or physician practice integration, CMS reduced the allocation of indirect PE for services performed in the hospital, believing those costs are now born by facilities. For services in the hospital setting, the portion of indirect PE allocated based on work RVUs will be reduced by 50% starting in 2026. This change will produce total RVU reductions of around 10% for facility-based services, such as pacemaker implants, TAVR, PCI, ablation, etc.
- Left Atrial Appendage Occlusion (LAAO): Despite efforts to delay revaluation of the LAAO code 33340 due to a restricted and flawed survey, CMS finalized the American Medical Association Relative Value Scale Update Committee (RUC)-recommended value of 10.25, a nearly 27% reduction from the current work RVU of 14.00. The ACC, Heart Rhythm Society, and Society for Cardiovascular Angiography & Interventions are currently resurveying this code for the next RUC meeting.
- PCI: The PCI code family was revised at CPT and then resurveyed at the RUC in April 2024 for implementation in 2026. CMS finalized the RUC-recommended values for all 12 codes. Several codes were reduced while others saw an increase in their work RVU. New codes were created for more complex stent cases and revascularization of a chronic total occlusion to allow for more accurate valuation.
- Lower Extremity Revascularization (LER): The LER code family was revised at CPT from 16 codes to 46 codes. All RUC-proposed values for the new codes were finalized. CMS may look to hospital outpatient cost data for practice expense in future rules.
- Remote Physiologic Monitoring: Several new remote monitoring codes were created and existing codes resurveyed. As these surveys did not reach the minimum response threshold, CMS will maintain the existing code values over the lower RUC recommendations and value the new codes using ratios related to those existing codes. The code family will be resurveyed in January 2028.
- Baroreflex Activation Therapy (BAT): Seven of the eight newly created codes for BAT are set at the RUC recommendations. One programming code was moderately reduced via crosswalk to an existing code. CMS adjusted clinical staff to be nurses for device interrogation and programming.
- Practice Expense: The rule finalized work and/or PE values for new/revised codes for LER, BAT, CT coronary plaque assessment and remote physiologic monitoring. More information is available in supporting data tables on values for these and all codes.
Your ACC Fights For Physician Payment, Opposes Looming Efficiency Adjustment
When the Centers for Medicare and Medicaid Services (CMS) released the 2026 Medicare PFS proposed rule earlier this summer, the ACC raised concerns over several policy changes projected to have a significant impact on payment for cardiovascular services. These efforts have continued as many of the proposed policies have now been finalized.
"While the 2026 Physician Fee Schedule includes an increase in Medicare reimbursement passed by Congress, it also relies on new and potentially disruptive payment policies that will significantly impact clinicians and patients during an already uncertain time in health care," said ACC President Christopher M. Kramer, MD, FACC.
"In particular, the ACC is concerned that CMS chose to keep the proposed changes to site of service payment differential and efficiency adjustment, despite widespread concerns from the medical community," he said. "These changes overlook the real overhead costs practices face and assume indefinite efficiency gains that could devalue essential services over time. These policies risk undermining practice sustainability across all specialties and limiting access to care for Medicare patients."
While CMS is applying a more than 3.5% increase to the conversion factor for 2026, this increase will be largely offset by the efficiency adjustment reduction that will disproportionately affect procedural and diagnostic services. Combined with the failure to account for significant inflation in practice costs, this move perpetuates long-term financial instability in the Medicare physician payment system, threatening patient access to Medicare-participating physicians and services.
The ACC, along with other medical societies, has aligned with the American Medical Association on a set of principles to guide advocacy efforts on Medicare physician payment reform. Earlier this year, the College joined other medical specialty organizations in a statement addressed to Congress urging long-term reform. Additionally, the ACC recently joined a letter to congressional leadership, requesting they stop implementation of the efficiency adjustment before Jan. 1, 2026.
In the previous Congress, legislation was introduced to include an annual inflationary update linked to the Medicare Economic Index and to raise the budget neutrality threshold to help reduce year-to-year cuts. The ACC is now working to introduce similar legislation in this Congress.
Learn more about ACC's ongoing efforts to establish sustainable Medicare payment practices.
Ambulatory Specialty Model For Heart Failure: Overview and Key Considerations
As part of the Medicare PFS final rule, the Centers for Medicare and Medicaid Services (CMS) is advancing its most significant and impactful demonstration project for cardiovascular clinicians to date. The Ambulatory Specialty Model (ASM) for heart failure (HF) is a five-year mandatory project aimed at evaluating, scoring and compensating cardiologists for the care of traditional Medicare beneficiaries with HF. The model will be implemented in to-be-selected geographic areas across the country starting Jan. 1, 2027, and will conclude at the end of 2031.
The ASM for HF borrows the existing framework of the Merit-based Incentive Payment System (MIPS) which includes four categories (quality, cost, improvement activities and improving interoperability) to assess participating cardiologists and distribute potential bonuses and penalties from +9% to –9% of their total Part B claims payments. Participant risk levels will increase by 1% each year in performance years 3 through 5.
Once mandatory geographic areas are selected, ASM participation will be limited to physicians with a PECOS-specialty of cardiology and have historically treated at least 20 HF patients per year, identified by the episode-based cost measure methodology. Other specialties likely caring for HF patients and nonphysician practitioners are excluded from the model.
Unlike MIPS, ASM intentionally excludes group or practice-level participation. Each physician will be required to submit the applicable data for each performance category. The performance assessment is based on the following:
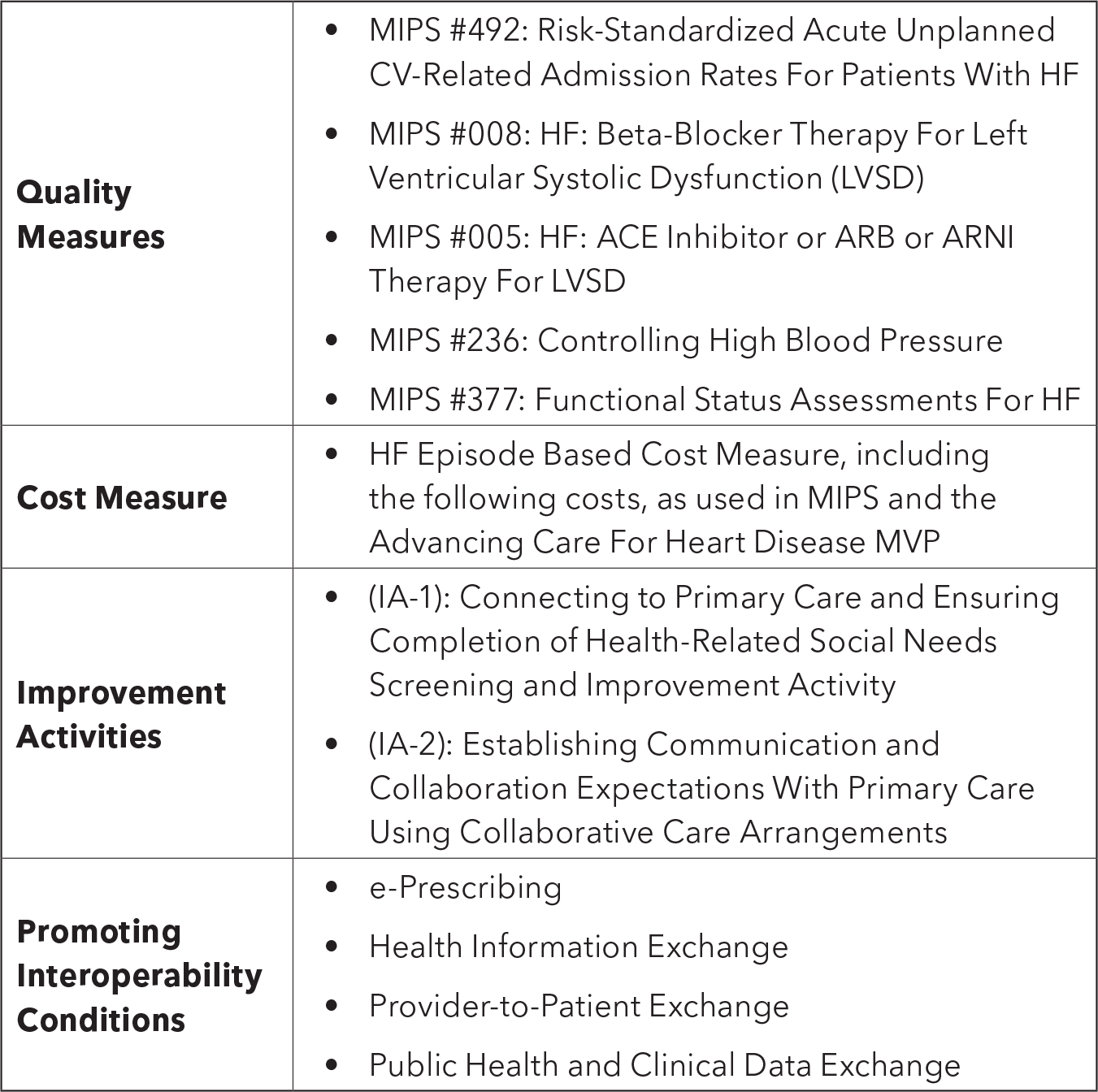
Each quality and cost measure will be weighted 50% of the final score. The improvement activities and promoting interoperability performance categories are added weights to broaden the distribution of final scores. The maximum scoring adjustment for improvement activities and promoting interoperability performance categories would be –20 points and –10 points, respectively.
Final scores will determine if participants receive positive, neutral or negative payment adjustments on future claims. Adjustments will be implemented two years after the applicable performance year.
As designed, the ASM excludes the active and important role of advanced practice practitioners, primary care and other specialties caring for HF patients, which the ACC highlighted as key concern in comments to CMS. Unfortunately, the agency made no significant changes when finalizing the rule.
The ACC will continue to solicit CMS for improvements and is committed to assisting members with this model through educational tools, webinars and Q&A sessions. Access the latest on the ASM for HF.

Clinical Topics: Heart Failure and Cardiomyopathies, Acute Heart Failure
Keywords: Cardiology Magazine, ACC Publications, Prospective Payment System, Health Policy, Heart Failure, ACC Advocacy, Centers for Medicare and Medicaid Services, U.S., CM-Dec-2025