New in Clinical Guidance | High Blood Pressure Focus of New ACC/AHA Guideline

Key Points
- About 50% of U.S. adults will develop high BP during their lifetime.
- High BP is the most prevalent and modifiable risk factor for cardiovascular disease and all-cause mortality. The overarching BP treatment goal is <130/80 mm Hg for all adults, with additional considerations.
- Lifestyle changes are strongly recommended to prevent or treat elevated BP and hypertension.
- The 2025 ACC/AHA High BP Guideline has a new way to calculate 10-year risk: PREVENT Equation instead of the Pooled Cohort Equation.
- In adults with BP ≥130/80 mm Hg and lower cardiovascular disease risk (defined by PREVENT <7.5%), it is recommended to start medication if 3 to 6 months of lifestyle changes fail to lower BP <130/80 mm Hg.
Hypertension represents one of the most common and potent cardiovascular risk factors globally, affecting approximately 31% of the adult population worldwide (1.4 billion people),1 including nearly 50% of U.S. adults.2 Unfortunately, despite prior success in improving blood pressure (BP) control, rates of uncontrolled hypertension have increased over the past decade, contributing to adverse cardiovascular events including myocardial infarction, heart failure and stroke, as well as renal failure and need for dialysis.3
Standards for BP control have evolved greatly over the last 50 years, with a growing understanding of the importance of lower target thresholds. In 2017, the ACC/American Heart Association (AHA) released their guideline which moved the target BP threshold from <140/90 mm Hg to <130/80 mm Hg for most adults.4 This decision was largely driven by new data from studies such as the SPRINT trial which reinforced the mantra that 'lower is better' when it comes to chronic BP management.5
The College, in conjunction with the AHA and other national societies, recently released their updated 2025 High Blood Pressure Guideline, reaffirming a target BP of <130/80 mmHg.6 The reason behind the lower threshold compared to historical standards is clear: for every 10 mm Hg reduction in systolic BP, patients experience a reduced risk of coronary heart disease (17%), stroke (27%), heart failure (28%), all major cardiovascular events (20%) and all-cause mortality (13%).7
While the threshold for target BP remains unchanged from the most recent prior guideline, numerous changes and updates merit attention. One of the most noticeable differences is the change from the Pooled Cohort Equation (PCE)8 to the PREVENT Equation9 for assessment of 10-year cardiovascular risk. The reason for this change stems from the PREVENT Equation's broad generalizability, reflective of the diverse population from which the score was derived. Specifically, following its release, concerns about underestimation of risk among some racial and ethnic groups were raised for the PCE.10 By comparison, the PREVENT Equation removed race in favor of other metrics including the social deprivation index.11 To that end, PREVENT was found to have improved 10-year risk prediction over other tools.11
Learn More: On-Demand Webinar
View a webinar on the new high BP guideline and what it means for your patients led by experts from ACC's Prevention of Cardiovascular Disease Member Section Council and Hypertension Work Group.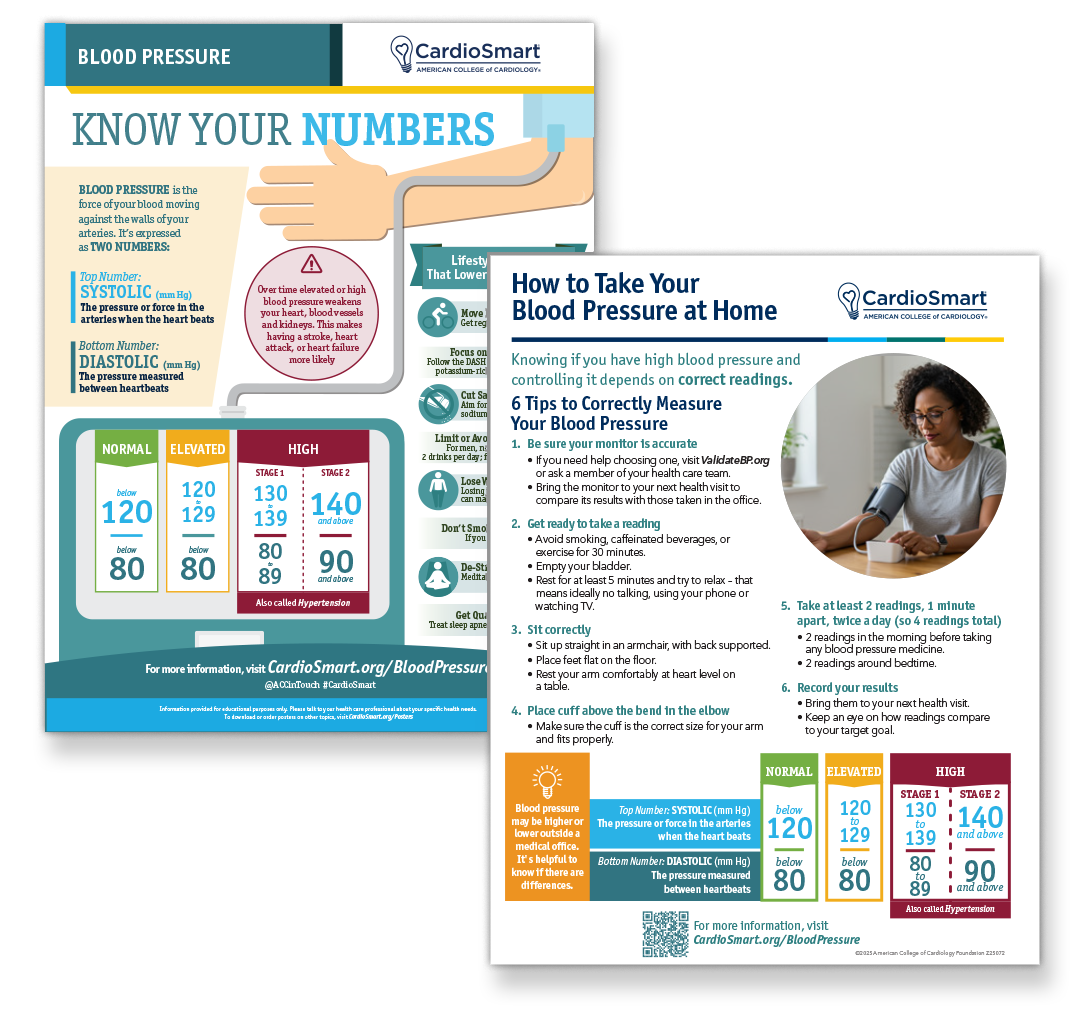
The 2025 High Blood Pressure Guideline now provides specific recommendations for patients with BP values between 130-139/80-89 mm Hg who are at lower 10-year risk, defined as an estimated risk of <7.5% by the PREVENT Equation. While patients in this category previously could remain in this BP range, the updated guideline now recommends pharmacotherapy to a target of <130/80 mm Hg if BP remains elevated despite three to six months of lifestyle modification.
Given the role of age in predicting 10-year cardiovascular risk, this update is likely to contribute to a larger number of younger patients receiving pharmacotherapy for elevated BP than under prior guidelines. This change reflects the established understanding the exposure to elevated BP, even by early to mid-life, is directly linked with increased risk of adverse cardiac outcomes in the future.12 In fact, hypertension onset before the age of 45 is associated with a more than twofold greater risk of cardiovascular disease and all-cause mortality.13
The new guideline also reaffirms the importance of a multidisciplinary approach to BP management, with involvement of a team of health care professionals to aid patients in achieving control. This team includes physicians, APPs, pharmacists, nutritionists and a myriad of other support staff to help diagnose, treat and maintain healthy BP levels.
Pharmacotherapy selection continues to highlight the first-line use of thiazide-type diuretics, long-acting dihydropyridine calcium channel blockers, and ACEI/ARBs, unless compelling reasons for other agents to be used first. Beyond medication selection, regimens should favor once a day dosing and the use of single pill combinations to improve medication adherence.14
The updated guideline also highlights the link between high BP and risk of cognitive impairment and dementia. Specifically, based on large meta-analyses, the guideline now gives a level 1A recommendation to achieving a systolic BP of <130 mm Hg to help reduce the risk of cognitive impairment and dementia.
Finally, following the publication of novel efficacy data, the updated guideline provides recommendations on the evaluation and clinical decision-making when considering renal denervation therapy for patients with resistant hypertension. Specifically, the guideline highlights the importance of a multidisciplinary approach to patient selection, removal of interfering medications, and shared decision-making prior to renal denervation therapy.
Overall, while the target threshold for most patients remains unchanged, the 2025 ACC/AHA High Blood Pressure Guideline offers nuanced guidance on achieving target BP thresholds, information on risk mitigation, and advice on how to best achieve optimal cardiovascular health for patients.
Scientific Statement Dives Into Risk Assessment For BP Management

Following the release of the 2025 multisociety High Blood Pressure Guideline, a new ACC/AHA Scientific Statement introduces the PREVENT model recommended in the guideline and details the supporting evidence and rationale behind its use.
PREVENT, which combines measures of cardiovascular, kidney and metabolic health, delivers more precise estimates of 10-year risk of total cardiovascular disease (including atherosclerotic cardiovascular disease and heart failure).

This article was authored by Joseph E. Ebinger, MD, FACC, Eugene Yang, MD, MS, FACC, and Eugenia Gianos, MD, FACC, all members of ACC's Prevention of Cardiovascular Disease Section.
References
- Mills KT, Stefanescu A, He J. The global epidemiology of hypertension. Nat Rev Nephrol 2020;16:223-37.
- Fryar CDK, Carroll B, Margaret D, et al. Hypertension prevalence, awareness, treatment, and control among adults age 18 and older: United States, August 2021-August 2023. National Center for Health Statistics (US) 2024.
- Peng X, Jin C, Song Q, et al. Stage 1 hypertension and the 10‐year and lifetime risk of cardiovascular disease: A prospective real‐world study. J Am Heart Assoc 2023;12:e028762.
- Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA Guideline for the Prevention, detection, evaluation, and management of high blood pressure in adults. JACC 2018;71:e127-e248.
- Lewis CE, Fine LJ, Beddhu S, et al. Final report of a trial of intensive versus standard blood-pressure control. N Engl J Med 2021;384:1921-30.
- Jones DW, Ferdinand KC, Taler SJ, et al. 2025 AHA/ACC guideline for the prevention, detection, evaluation, and management of high blood pressure in adults. JACC 2025;Epublished Aug 14.
- Ettehad D, Emdin CA, Kiran A, et al. Blood pressure lowering for prevention of cardiovascular disease and death: a systematic review and meta-analysis. Lancet 2016;387:957-67.
- Goff DC, Jr., Lloyd-Jones DM, Bennett G, et al. 2013 ACC/AHA guideline on the assessment of cardiovascular risk. Circulation 2014;129:S49-73.
- Khan SS, Matsushita K, Sang Y, et al. Development and validation of the American Heart Association's PREVENT Equations. Circulation 2024;149:430-49.
- Patel AP, Wang M, Kartoun U, et al. Quantifying and understanding the higher risk of atherosclerotic cardiovascular disease among south asian individuals: Results from the UK Biobank prospective cohort study. Circulation 2021;144:410-22.
- Zhou H, Zhang Y, Zhou MM, et al. Evaluation and comparison of the PREVENT and pooled cohort equations for 10-year atherosclerotic cardiovascular risk prediction. J Am Heart Assoc 2025;14:e039454.
- Suvila K, McCabe EL, Lehtonen A, et al. Early onset hypertension is associated with hypertensive end-organ damage already by midLife. Hypertension 2019;74:305-312.
- Wang C, Yuan Y, Zheng M, et al. Association of age of onset of hypertension with cardiovascular diseases and mortality. JACC 2020;75:2921-30.
- Parati G, Kjeldsen S, Coca A, et al. Adherence to single-pill versus free-equivalent combination therapy in hypertension. Hypertension 2021;77:692-705.
Clinical Topics: Prevention, Hypertension
Keywords: Cardiology Magazine, ACC Publications, American Heart Association, Blood Pressure, Practice Guideline, Hypertension