
From the Member Sections | Closing the Gap in Cardiology Competency in Peripheral Vascular Care
Peripheral artery disease (PAD) affects the lives of an estimated 21 to 27 million Americans.1 It is a misconception that PAD comes in isolation; in fact, most patients (>60-70%) also have concomitant coronary artery disease and/or cerebrovascular disease.2 Additionally, chronic venous diseases are far more prevalent than PAD, with estimates suggesting it affects five- to seven-times more individuals.3,4 Beyond the sheer numbers, the profound impact on outcomes and quality of life underscores the need for our specialty to expand the "vascular" component of cardiovascular disease training – and think more broadly in terms of peripheral vascular disease (PVD).
Current fellowship training provides the knowledge to reduce cardiovascular risk and board certification demands expertise in evidence-based cardiovascular risk-reduction strategies. Yet, clinical awareness of PVD remains limited across many cardiovascular disease training programs.
Implementing a more holistic approach on rounds – listening to the heart along with examining the limbs – could dramatically improve patient outcomes. Diminished ankle-brachial indices have long been known to be an independent predictor for cardiovascular mortality.5 While clinicians cannot place our fingers directly on a coronary artery, we can easily palpate a pedal pulse – an action that may help avert major adverse cardiovascular events. To quote Craig Walker, MD, a prolific interventional cardiologist and PVD fellowship program director at the Cardiovascular Institute of the South in Houma, LA: "Sick legs are never attached to healthy people."
For many patients, access to vascular care remains a major barrier. In many regions of the U.S., there are vascular care deserts where patients must travel hours to see a qualified vascular specialist such as a vascular surgeon or interventional radiologist. In contrast, cardiologists are far more accessible due to widespread availability of PCI-capable facilities. What is lacking, however, are interventional cardiologists with dedicated training in chronic limb threatening ischemia (CLTI) or venous disorders. Interventional cardiology programs increasingly emphasize invasive therapies for pulmonary embolism. Likewise, a substantial need exists to deepen our fellows' understanding of acute and chronic deep vein thrombosis and management of venous ulcers. Post-thrombotic syndrome is widely underappreciated, despite substantial morbidity and impact on quality of life.6
Interventional cardiology has played a foundational role in the development of modern endovascular techniques. The cornerstone of every peripheral intervention, balloon angioplasty, was invented by the German cardiologist Andreas R. Gruentzig, MD, FACC. Notably, in 1974 he first used his single-lumen peripheral balloon angioplasty catheter to dilate a patient's superficial femoral artery,7 preceding his creation of the field of percutaneous transluminal coronary angioplasty.
Atherectomy is another tool that has a cardiology footprint. Commonly employed today in peripheral interventions to debulk or modify atheromatous plaque in peripheral arteries, it received its first approval to treat peripheral arteries, after its development in 1985 by interventional cardiologist John B. Simpson, MD, PhD.
Today structural heart interventions dominate much of the enthusiasm within the field. However, without question, PVD far outweighs structural heart disease in terms of overall disease prevalence.
Consequently, there is very high demand for skilled endovascular specialists. Interventional cardiologists are uniquely geared for a career as a PVD specialist given their background in cardiovascular disease prevention and interventional skill set. It is mandatory that interventional cardiologists have "good hands," wire skills and clinical judgment during percutaneous coronary intervention. These baseline skills provide an excellent foundation to build on to perform CLTI interventions that often require below-the-knee or even below-the-ankle intervention for limb salvage.
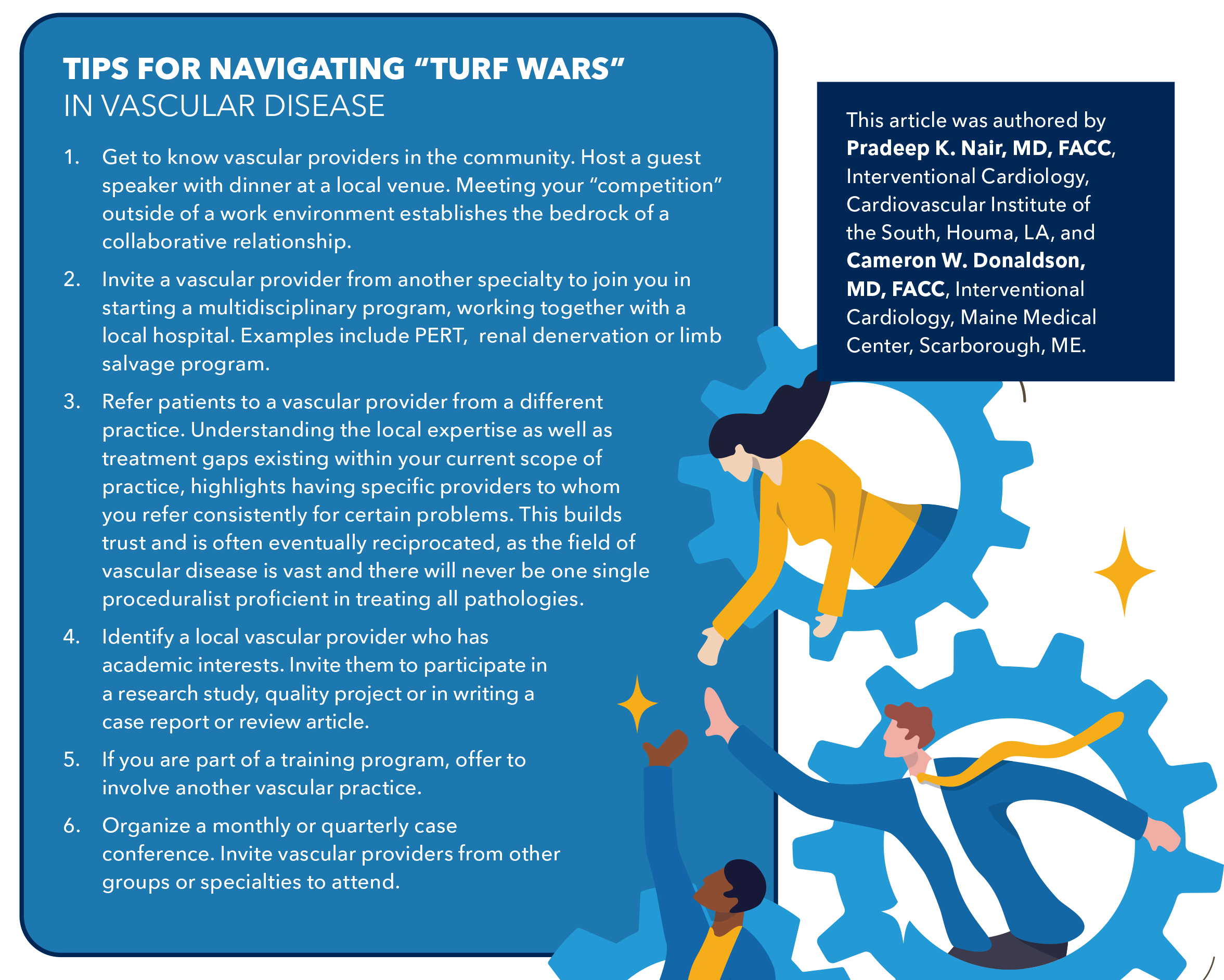
While many interventional cardiology programs may lack dedicated PVD training, there are several avenues for acquiring expertise. Trainees must commit to becoming true specialists rather than clinicians who "dabble" in peripheral intervention. Mastery leads to better patient outcomes and reduces scrutiny from non-cardiology vascular specialists. Although turf battles amongst vascular specialists remain an unfortunate reality, the greatest asset in such environments is unquestioned technical expertise backed by comprehensive training.
Surgery will always remain essential to vascular care, but so too will interventional and cardiovascular management. Over time, if the sincerity and dedication to improving vascular care is present, the hope is that collegiality and cooperation will win out for the betterment of patients.
Becoming an Expert in PVD Intervention
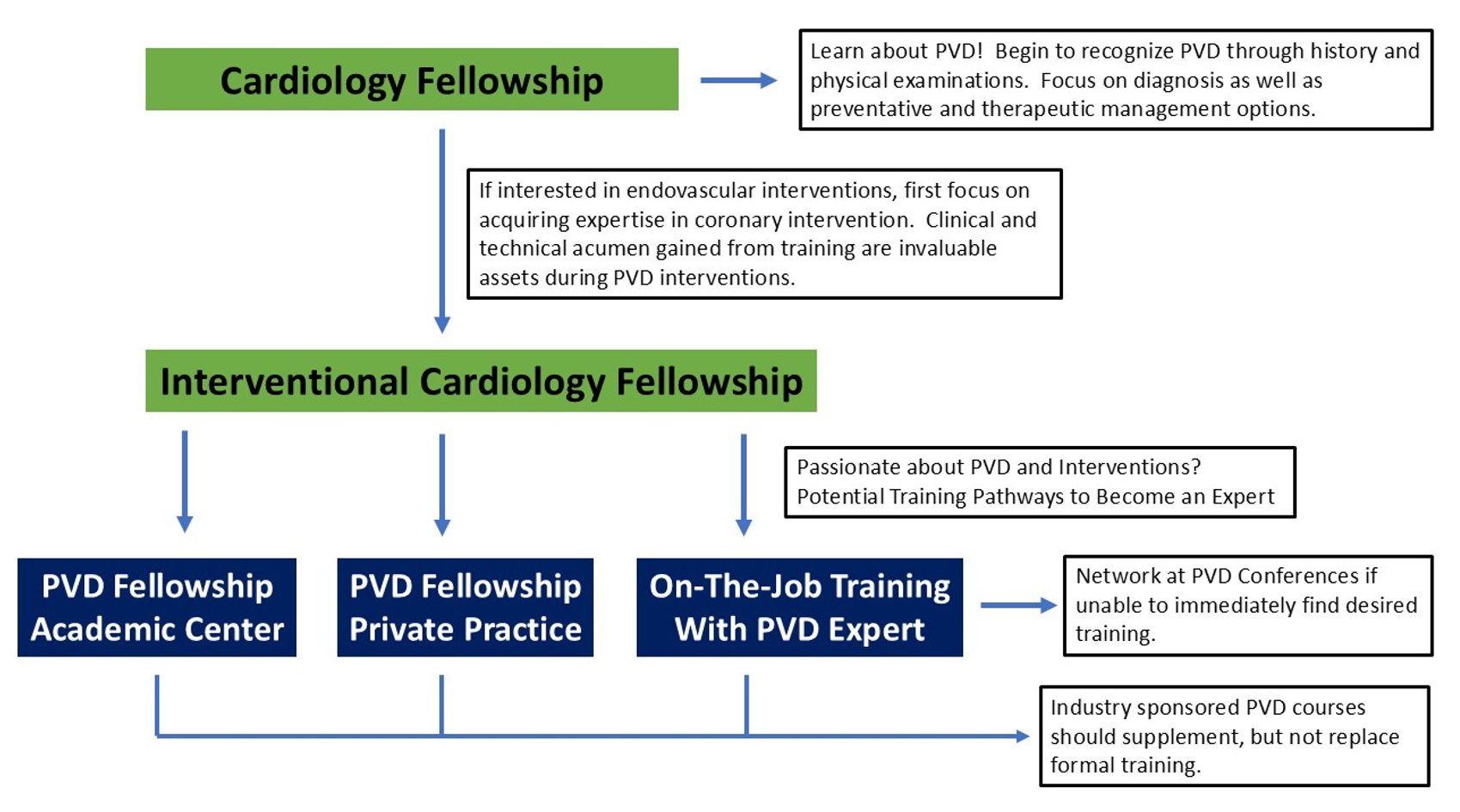
How, then, does a cardiologist become an expert in PVD intervention? While PVD-focused training is not accredited by the Accreditation Council for Graduate Medical Education (ACGME), multiple cardiology programs offer dedicated PVD fellowships, housed either at major academic centers or led by prominent interventional cardiologists in private practice.
Another viable path involves joining a practice with established endovascular specialists willing to train motivated early-career providers. During such non-ACGME training, safeguards to ensure income stability are essential; voluntary or unpaid roles should be considered only as a last resort, given the level of training these applicants already possess. If immediate training opportunities are not available, continued engagement through networking at PVD-focused conferences can significantly increase the likelihood of securing advanced instruction. Industry sponsored courses provide useful exposure but should supplement – not replace – formal fellowship or structured on-the-job training.
In essence, this is a call to action for cardiology fellowship program directors, fellows and early-career interventional cardiologists. By expanding our focus more deliberately into the realm of PVD, our specialty can profoundly influence disease progression and improve the lives of millions of patients.
Cardiology Training Pathways to Become a Dedicated Specialist in Peripheral Vascular Disease and Interventions
Editors' Note: This is the second article in a two-part series on PVD. Read the first article in the December 2025 issue.
References
- Yost ML. The current U.S. prevalence of peripheral artery disease. Vascular Disease Management. 2023;20:E67-E73.
- Mahoney EM, Wang K, Keo HH, et al. Vascular hospitalization rates and costs in patients with peripheral artery disease in the United States. Circ Cardiovasc Qual Outcomes. 2010;3:642-51.
- Attaran RR, Carr JG. Chronic venous disease of the lower extremities: a state-of-the art review. J Soc Cardiovasc Angiogr Interv. 2022;2:100538.
- Yost M. 2025. Chronic Venous Disease (CVD), Epidemiology, Costs and Consequences. The SAGE Group. Available here.
- Newman AB, Shemanski L, Manolio TA, et al. Ankle-arm index as a predictor of cardiovascular disease and mortality in the cardiovascular health study. Arterioscler Thromb Vasc Biol 1999;19:538-45.
- Chaitidis N, Kokkinidis DG, Papadopoulou Z, et al. Management of post-thrombotic syndrome: a comprehensive review. Curr Pharm Des. 2022;28:550-59.
- Gruentzig A. Perkutane rekanalisation chronischer arterieller verschlusse mit einem neuen dilationskatheter modification der Dotter Technik. Deutsh Med Wochenschr. 1974;99:2502-2510.
Clinical Topics: Invasive Cardiovascular Angiography and Intervention, Vascular Medicine, Atherosclerotic Disease (CAD/PAD), Interventions and Vascular Medicine
Keywords: Cardiology Magazine, ACC Publications, CM-Jan-Feb-2026, Peripheral Arterial Disease, Percutaneous Coronary Intervention, Vascular Diseases, Ischemia, Education