
Peripheral Matters | Inferior Vena Cava Filter Retrieval: Update on Advanced Techniques
Inferior vena cava (IVC) filters are indicated for the prevention of pulmonary embolism in patients with lower-extremity deep vein thrombosis when there is a contraindication to anticoagulation. In the U.S., IVC filter placement increased nearly 25-fold from the 1980s to early 2000s, primarily driven by the clearance of retrievable filters by the U.S. Food and Drug Administration (FDA).1 Expanded indications, including for thromboprophylaxis, drove increased utilization as well.2 However, despite this increase and the option for retrievability, <10% of filters are retrieved once the risk of pulmonary embolism has subsided.3
Although retrievable, IVC filters are approved for permanent implantation. In the late 2000s, trends emerged suggesting that these specific devices were subject to device-related complications, including filter fracture, migration, penetration of adjacent organs, and additional thromboembolic events; this was positively correlated with extended implantation time.4
A review of the FDA Manufacturer and User Facility Device Experience (MAUDE) database demonstrated that device-related adverse events associated with retrievable filters were reported at greater frequency relative to permanent filters.5 This led the FDA to issue safety communications in 2010 and 2014, advocating active surveillance of patients with retrievable IVC filters in place, with consideration for retrieval when clinically appropriate. This was followed by a 2020 multisociety consensus statement, including the Society of Interventional Radiology, the ACC and the Society for Vascular Surgery, advocating retrieval of IVC filters if benefits outweigh clinical risk.6
In addition to a higher risk of device-related complications, extended implantation time is associated with increased failure of standard retrieval techniques.7 The development of advanced retrieval techniques has had a positive impact on filter retrieval, with downstream mitigation of device-related filter complications.8
Retrieval Workup and Non-Laser Advanced Retrieval Techniques
Preprocedural planning is paramount, especially for devices with extended implantation times. We have a standardized methodology for triage of patients, including assessment of various device-related complications that are identified on preprocedure imaging.9 In our practice, we review a computed tomographic scan of the abdomen/pelvis. This allows for identification of device type, adequate assessment for filter tilt, fracture, caval penetration including involvement of adjacent organs, or the presence of caval thrombosis.
All filter removal procedures should begin with initial cavography to assess for thrombus; we typically place a pigtail catheter caudal to the filter and perform a power injection. Standard retrieval techniques consist of engaging the apex or hook of the filter using an endovascular snare, followed by co-axial collapse of the filter into a sheath.
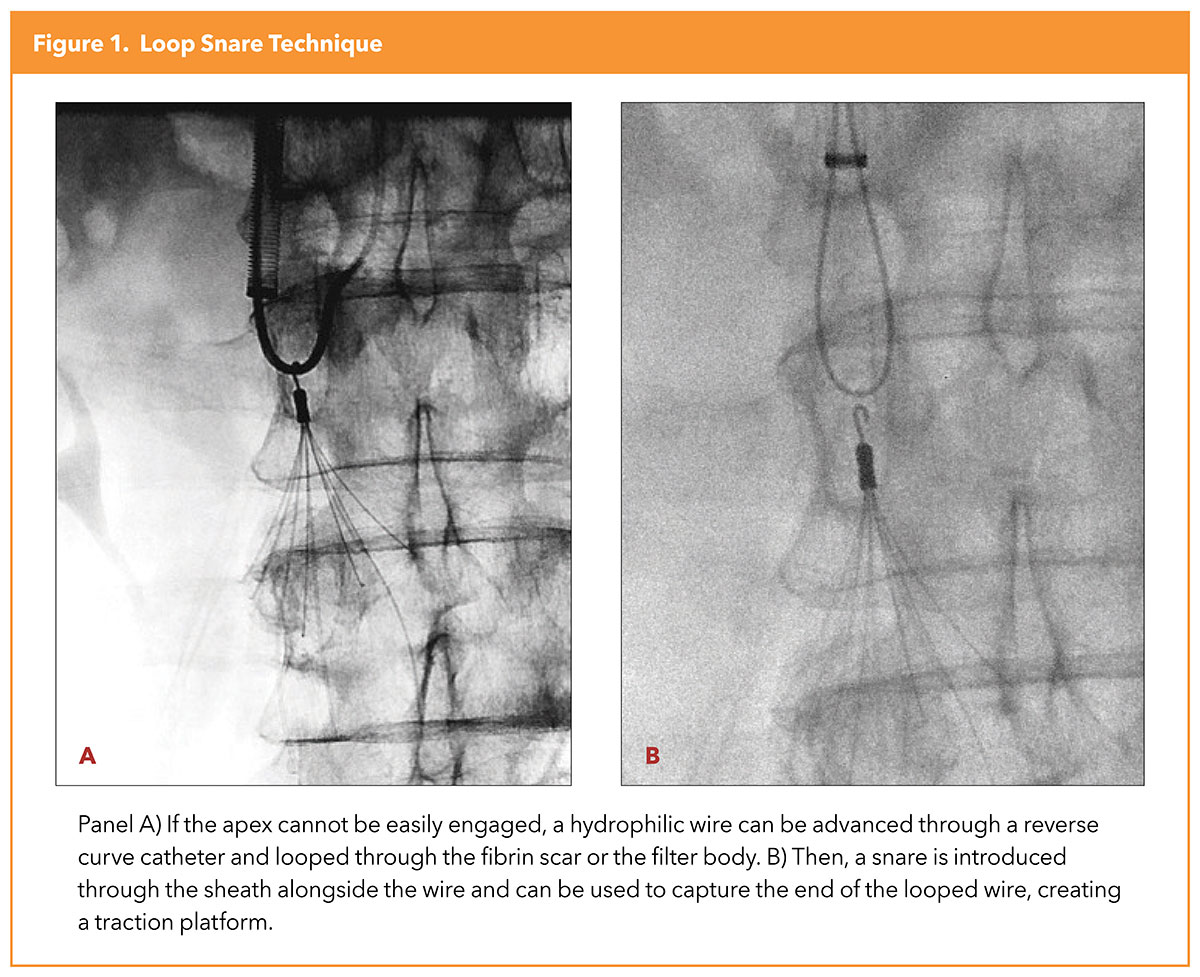
If the apex cannot be captured, usually due to encasement in scar along the caval wall, several options are available to gain control of the filter apex/hook. The loop snare technique is widely used, whereby a hydrophilic wire is advanced through a reverse curve catheter and looped through the scar, or less frequently, the filter body itself. An endovascular snare is then introduced through the sheath, alongside the wire, used to capture the end of the looped wire which is then externalized. The looped wire now serves as a traction platform, and countertraction is applied via the sheath to collapse and retrieve the filter (Figure 1).10
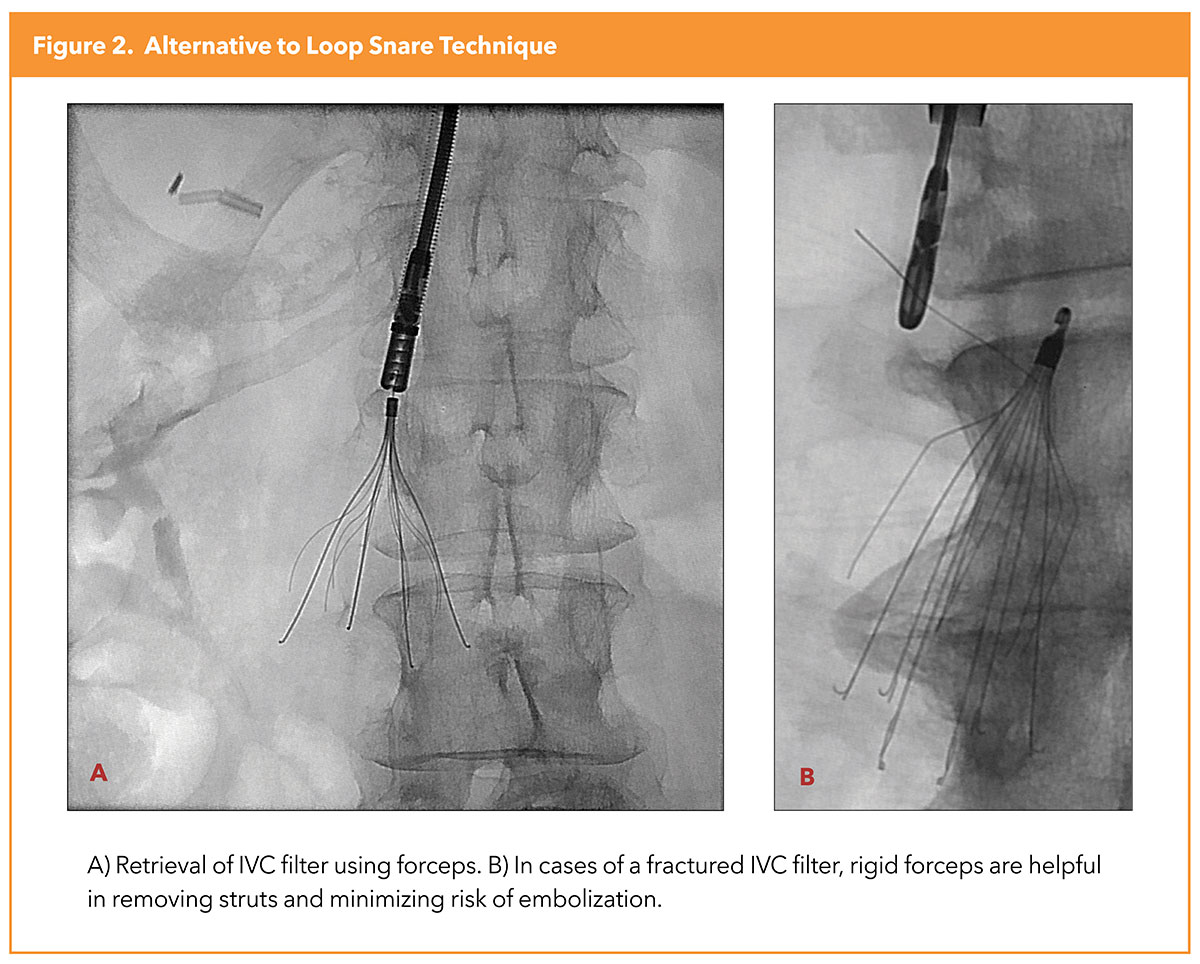
An alternative to the loop snare is the off-label use of rigid endobronchial forceps (model 4162, Lymol Medical Corporation, Woburn, MA) (Figure 2).11 This technique has become our favored approach to embedded apices. These forceps are malleable to achieve an optimal shape. Forceps may also be used to retrieve fractured intraluminal struts, thereby mitigating the risk of future embolization. A 12Fr sheath is the minimal size needed for use of forceps; we frequently use a 16Fr sheath. When using forceps, it is favored that the patient is under deep sedation or general anesthesia as the procedure can cause discomfort. Additionally, inadvertent trauma to the IVC wall can occur; thus, operator experience is critical.
Excimer Laser Sheath-Assisted Retrieval
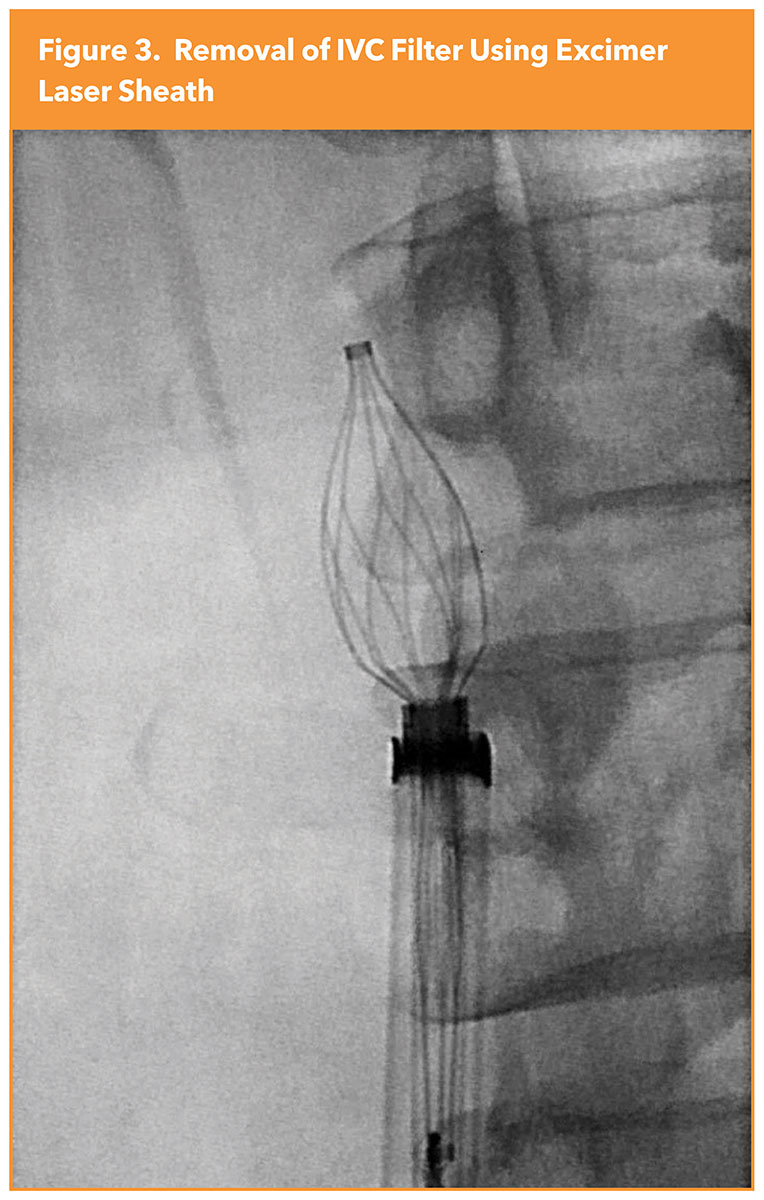
When IVC filter struts become incorporated into the caval wall due to fibrosis, extensive traction forces are frequently required, which may be hazardous and result in caval trauma. Laser sheaths, traditionally used for pacemaker or defibrillator lead extraction, have been successfully used as an adjunctive advanced method to remove embedded filters through the application of cool ultraviolet laser technology to photothermally ablate the tissue encasing filters, thereby reducing the traction forces required to retrieve the filter and improving the safety profile of the procedure (Figure 3).12
Our group demonstrated in 2020 that the 308-nm XeCl excimer laser sheath (14Fr/16Fr CavaClear, Philips/Spectranetics, Colorado Springs, CO) is particularly useful for IVC filters with "closed-cell" designs whose complete metal or wire circuits facilitate greater IVC incorporation due to increased surface area contact with the caval wall. Among 441 patients, closed-cell filters, prolonged dwell times and prior failed retrieval attempts, were predictive of the need for laser-facilitated retrieval.13
In 2021, the FDA approved CavaClear as the first device specifically indicated for complex IVC filter retrieval. Most recently, a multicenter cohort reinforced the use of the laser sheath for retrieval of embedded IVC filters, suggesting broader applicability of the procedure, corroborating previous single-center studies.12-14 Among seven centers with varying degrees of volume and expertise, the primary safety endpoint of device-related major complication rate occurred in <3% of procedures, with no complication independently adjudicated to be definitively related to the use of the laser sheath. The technical success rate for IVC filter retrieval with the laser sheath was 95.2%.14
Future Directions
Despite ever-increasing awareness of best practices for filter retrieval, the high prevalence of filters with extended implantation times requires awareness of advanced retrieval techniques. An increasing body of literature demonstrates that when done correctly, advanced techniques using the excimer laser sheath is safe and effective for retrieval of filters regardless of implantation time.15
Given more recent data on the broader applicability of laser technology, there needs to be parallel efforts to boost expertise in other advanced retrieval techniques, as more than one technique is frequently necessary. As the armamentarium and awareness for filter retrieval grows, a shift in the practice paradigm could result in future positive outcomes for the thousands of filter-bearing patients.


This article was authored by Shin Mei Chan, BS, Yale School of Medicine, New Haven, CT, and Kush R. Desai, MD, Department of Radiology, Northwestern University Feinberg School of Medicine, Chicago, IL.
References
- Stein PD, Matta F, Hull RD. Increasing use of vena cava filters for prevention of pulmonary embolism. Am J Med 2011;124:655-61.
- Wang SL, Lloyd AJ. Clinical review: Inferior vena cava filters in the age of patient-centered outcomes. Ann Med 2013;45:474-81.
- Mohapatra A, Liang NL, Chaer RA, Tzeng E. Persistently low inferior vena cava filter retrieval rates in a population-based cohort. J Vasc Surg Venous Lymphat Disord 2019;7:38-44.
- McLoney ED, Krishnasamy VP, Castle JC, et al. Complications of Celect, Gunther tulip, and Greenfield inferior vena cava filters on CT follow-up: A single-institution experience. J Vasc Interv Radiol 2013;24:1723-9.
- Andreoli JM, Lewandowski RJ, Vogelzang RL, Ryu RK. Comparison of complication rates associated with permanent and retrievable inferior vena cava filters: A review of the MAUDE database. J Vasc Interv Radiol 2014;25:1181-5.
- Kaufman JA, Barnes GD, Chaer RA, et al. Society of Interventional Radiology clinical practice guideline for inferior vena cava filters in the treatment of patients with venous thromboembolic disease: Developed in collaboration with the American College of Cardiology, American College of Chest Physicians, American College of Surgeons Committee on Trauma, American Heart Association, Society for Vascular Surgery, and Society for Vascular Medicine. J Vasc Interv Radiol 2020;31:1529-44.
- Desai KR, Laws JL, Salem R, et al. Defining prolonged dwell time: When are advanced inferior vena cava filter retrieval techniques necessary? An analysis in 762 procedures. Circ Cardiovasc Interv 2017;10(6) e003957.
- Desai KR, Pandhi MB, Seedial SM, et al. Retrievable IVC filters: Comprehensive review of device-related complications and advanced retrieval techniques. Radiographics 2017;37:1236-45.
- Grewal S, Lewandowski RJ, Ryu RKW, Desai KR. Inferior vena cava filter retrieval: Patient selection, procedural planning, and postprocedural complications. AJR Am J Roentgenol 2020;215:790-4.
- Al-Hakim R, McWilliams JP, Derry W, Kee ST. The hangman technique: A modified loop snare technique for the retrieval of inferior vena cava filters with embedded hooks. J Vasc Interv Radiol 2015;26:107-10.
- White SB, Stavropoulos SW. Retrieval of a wall-embedded recovery inferior vena cava filter using rigid bronchoscopy forceps. Semin Intervent Radiol 2007;24:15-9.
- Kuo WT, Doshi AA, Ponting JM, et al. Laser-assisted removal of embedded vena cava filters: A first-in-human escalation trial in 500 patients refractory to high-force retrieval. J Am Heart Assoc 2020;9):e017916.
- Desai KR, Xiao N, Salem R, et al. Excimer laser sheath-assisted retrieval of "closed-cell" design inferior vena cava filters. J Am Heart Assoc 2020;9:e017240.
- Desai KR, Kaufman J, Truong P, et al. Safety and success rates of excimer laser sheath-assisted retrieval of embedded inferior vena cava filters. JAMA Netw Open 2022;5:e2248159.
- Desai KR, Lewandowski RJ, Salem R, et al. Retrieval of inferior vena cava filters with prolonged dwell time: A single-center experience in 648 retrieval procedures. JAMA Intern Med 2015;175:1572-4.
Clinical Topics: Anticoagulation Management, Arrhythmias and Clinical EP, Cardiac Surgery, Cardiovascular Care Team, Pulmonary Hypertension and Venous Thromboembolism, Vascular Medicine, Anticoagulation Management and Venothromboembolism, Implantable Devices, SCD/Ventricular Arrhythmias, Cardiac Surgery and Arrhythmias
Keywords: ACC Publications, Cardiology Magazine, Anticoagulants, Triage, Cicatrix, Radiology, Interventional, Prevalence, Traction, United States Food and Drug Administration, Off-Label Use, Venous Thromboembolism, Venous Thrombosis, Pulmonary Embolism, Thrombosis, Surgical Instruments, Pacemaker, Artificial, Contraindications, Catheters, Defibrillators, Extremities, Abdomen, Pelvis, Multicenter Studies as Topic, Vena Cava Filters
< Back to Listings
