
For the FITs | Closing the Mortality Gap For People Living With HIV: Updated Recommendations For Statins For Primary Prevention of ASCVD

An estimated 1.2 million people in the U.S. are living with human immunodeficiency virus (HIV).1 Since the introduction of antiretroviral therapy (ART) almost three decades ago, life expectancy has dramatically improved for HIV-positive patients. With the epidemiologic transition of HIV to a chronic disease, more individuals are living longer with a high burden of comorbid illness, including atherosclerotic cardiovascular disease (ASCVD).2-4
Patients living with HIV (PLWH) have an almost two-fold increased risk of myocardial infarction (MI) and heart failure (HF) compared to the general population.5-7 ASCVD is a leading cause of morbidity among this population and remains a major reason a gap in life expectancy still exists for PLWH.8
PLWH not only have a higher incidence of ASCVD, disease manifests earlier and tends to be more aggressive, even among individuals with sustained viral suppression. This increased risk can be attributed to both traditional and HIV-specific risk factors.9
Inflammation is a major driver of ASCVD pathogenesis, beginning with immune-mediated injury of endothelial cells.10 Chronic HIV results in a persistent inflammatory state and accelerates plaque formation through abnormal activation of both adaptive and innate immune pathways.11-13
Although early diagnosis and initiation of ART remains a fundamental step for prompt viral suppression and restoration of normal immunity, a degree of abnormal inflammation still exists.11-14 Coronary microvascular dysfunction is also considered a potential mechanism of accelerated ASCVD among PLWH through chronic inflammation leading to endothelial activation and dysfunction.15
Original ART regimens were initially hypothesized to contribute to elevated MI risk among PLWH, however more modern regimens including integrase inhibitors, have proven to be more favorable despite causing some weight gain.16 As HIV viremia and low CD4+ cell count are strongly associated with accelerated ASCVD and HF, prompt initiation of ART is essential for both cardioprotective benefits and optimal HIV care.17-19
New Course on HIV and Lifelong Care
The HIV and Lifelong Care Course from ACC's NCD Academy explores the relationship between HIV/AIDS and noncommunicable diseases (NCDs), the impact of ART, and more. Visit ACC.org/NCDAcademy to access this course.

Resources
Click here to download the HHS recommendations for statins in people living with HIV.
Click here to access the HHS HIV Clinical Guidelines.
Primary prevention 10-year risk calculators commonly used among primary care providers and specialists, such as the ACC/AHA ASCVD Risk Calculator and AHA PREVENT Calculator, include traditional risk factors such as body mass index, renal function, diabetes, hypertension and smoking history among others. HIV is considered a risk-enhancer, yet it is not included in these estimates. As a result, regardless of the risk estimate including these traditional risk factors, the true risk of ASCVD among PLWH is much higher.9
This risk can be further underestimated for those with viral co-infections (such as Hepatitis C or cytomegalovirus), prolonged viremia or a strong family history.16
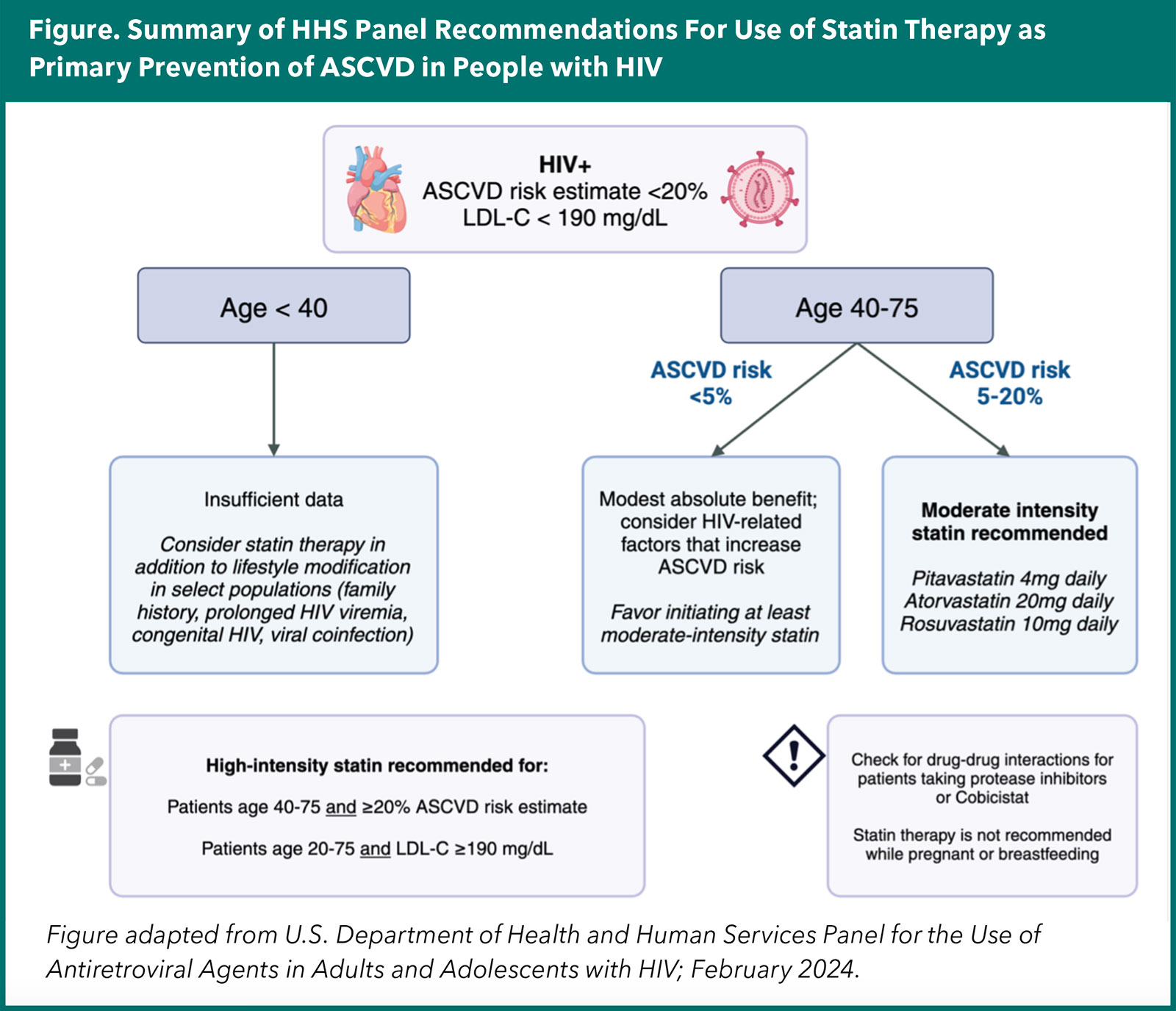
Health disparities and structural barriers in screening PLWH likely exist and can contribute to heightened disease burden. The following cases will help to highlight updated recommendations for statin use from the U.S. Department of Health and Human Services (HHS) Panel for the Use of Antiretroviral Agents in Adults and Adolescents with HIV in collaboration with the ACC, American Heart Association and HIV Medicine Association and published in February 2024.20
Case 1
Ms. C is a 43-year-old woman with well-controlled HIV for six years on Biktarvy (bictegravir, emtricitabine, tenofovir alafenamide). Her 10-year ASCVD risk score is between 5-7.5% based on traditional risk factors.
Recommendation
REPRIEVE (Pitavastatin to Prevent Cardiovascular Disease in HIV Infection), a large, phase 3, global trial, randomly assigned 7,769 patients with HIV on ART and low-to-moderate risk of ASCVD to receive daily pitavastatin or placebo.21 Participants were a median of 50 years old (IQR 45-55) and 41% Black, with a low-moderate ASCVD risk score (10-year risk 4.5% and median LDL 107 mg/dL) and well-controlled HIV (median CD4 cell count 621 cells/mm3 and HIV viral load undetectable in 88%). REPRIEVE was stopped early for efficacy after a median follow-up of 5.1 years.
The statin arm was associated with a 35% reduction in major adverse cardiovascular events (hazard ratio [HR], 0.65; 95% CI, 0.48-0.90), which was particularly pronounced for patients with ASCVD risk estimates ≥5% compared to <5%. Results were consistent across subgroups, including country, further emphasizing the global burden of heightened ASCVD risk among PLWH.
The REPRIEVE study helped demonstrate the benefits of statin therapy for primary prevention among PLWH and low-to-intermediate ASCVD risk (<20%). The absolute risk reduction was larger than what would be expected from LDL-lowering properties alone, potentially attributed to additional treatment effects on inflammatory pathways.22
The panel recommends initiating at least a moderate-intensity statin for patients aged 40-75 years with 10-year ASCVD risk estimates between 5-20% (Figure). Moderate intensity statins include pitavastatin 4 mg, atorvastatin 20 mg or rosuvastatin 10 mg once daily.
Case 2
Mr. J is a 55-year-old man with HIV on a protease inhibitor-based regimen which includes darunavir boosted with ritonavir. His 10-year ASCVD risk estimator is around 15% based on traditional risk factors.
Recommendation
Based on the Panel recommendations and the results of the REPRIEVE study, this patient also meets criteria for at least a moderate-intensity statin given his low to intermediate 10-year ASCVD risk. However, it is important to recognize the drug-drug interactions with a protease-inhibitor-based ART regimen. Ritonavir- and cobicistat-boosted regimens are most susceptible to interactions with statin therapy due to cytochrome P450 metabolism.20
Atorvastatin, lovastatin and simvastatin are primarily metabolized by CYP3A4, resulting in increased statin exposure.23 The panel recommends atorvastatin dose reduction and increased monitoring for adverse effects with co-administration. Lovastatin and simvastatin are contraindicated with ritonavir- or cobicistat-boosted ART.
Pitavastatin, pravastatin and rosuvastatin are not primarily metabolized by the CYP pathway, however fluctuations in statin concentrations can still be seen with various ART.23 Rosuvastatin 10 mg once daily would be the recommended initial statin therapy for this patient with careful monitoring for adverse effects and not to exceed 20 mg as increased concentrations can be observed with co-administration. Pravastatin is also more commonly used for patients on ART to avoid drug-drug interactions but would not be recommended in this patient as it is only considered a low-intensity statin due to decreased bioavailability.23
Management of ART and drug interactions will vary from patient to patient. Moreover, the Panel recommends careful attention to drug interactions for patients on protease inhibitors, cobicistat-boosted therapy, older non-nucleoside reverse transcriptase inhibitors (e.g., efavirenz) and atypical regimens for patients with resistant HIV infection (including fostemsavir and lenacapavir). The HIV Clinical Guidelines offer a robust list of drug interaction information and recommendations for statin adjustments that can be easily accessed for safe treatment options.24
Case 3
Ms. S is a 34-year-old woman with HIV diagnosed fifteen years ago. She started ART with Dovato (dolutegravir and lamivudine) in the past year. She was also diagnosed with Hepatitis C and is awaiting treatment initiation; her LDL serum level is 105 mg/dL and her father had an MI at age 48.
Recommendation
This patient represents a young woman with longstanding HIV and increased ASCVD risk based on multiple HIV-related and traditional risk factors. The REPRIEVE trial enrolled patients over 40 years of age, thus the Panel offers different considerations for a younger age category. Similar to the general population, lifestyle modification is first recommended, however some individuals are still considered at elevated ASCVD risk.
For patients with a family history of premature ASCVD, familial hypercholesterolemia or prolonged duration of HIV infection (including congenital HIV or prolonged HIV viremia), earlier statin therapy should be considered. Additionally, patients with viral co-infection, including Hepatitis C, have ongoing immune activation and may also be at higher risk for accelerated ASCVD.4,17
The decision to initiate statin therapy in PLWH under 40 years of age should be considered on an individual basis yet should not be overlooked as ASCVD develops earlier and can be more aggressive in this population.25,26
The overall risk of adverse effects of statin therapy are minimal, most commonly muscle-related symptoms and more rarely transient rises in liver enzymes or new-onset diabetes. The statin arm of the REPRIEVE study demonstrated small increases in muscle-related symptoms (2.3% vs. 1.4% with placebo) and new-onset diabetes (5.3% vs. 4.0% with placebo).21
Shared decision-making between the physician and patient should include discussions with regard to the benefits and favorable safety profile of statins, in addition to assessing additional risk-factors for diabetes.27,28
As previously mentioned, careful attention should be made for monitoring adverse effects in patients taking protease inhibitors and cobicistat-boosted ART. For this patient, drug interactions must also be considered between statin therapy and Hepatitis C treatment options.
Conclusion
HIV is considered a risk-enhancer for development of ASCVD, resulting in an underestimation of 10-year ASCVD risk estimates and delayed intervention for PLWH. The gap in life expectancy is closing with the refinement of ART, however ASCVD remains a leading cause of morbidity and mortality.
The results of the REPRIEVE trial have led to concise recommendations for the use of statin therapy for PLWH. Enhanced education for providers will help to expand screening and initiation of appropriate primary prevention therapies, ultimately lessening the health disparities and closing the mortality gap for PLWH.
This article was authored by Elena M. Donald, MD, a fellow-in-training in Adult Cardiovascular Disease at Columbia University Irving Medical Center-New York Presbyterian Hospital, and FIT Section editor. Reach out to her with story ideas via @elenadonaldMD or cardiologyeditor@acc.org.
References
- Hall HI, Song R, Tang T, et al. HIV trends in the United States: diagnoses and estimated incidence. JMIR Public Health Surveill 2017;3:e8.
- Collaboration H-C, Ray M, Logan R, et al. The effect of combined antiretroviral therapy on the overall mortality of HIV-infected individuals. AIDS 2010;24:123-37.
- Uriel N, Nahumi N, Colombo PC, et al. Advanced heart failure in patients infected with human immunodeficiency virus: is there equal access to care? J Heart Lung Transplant 2014;33:924-30.
- Feinstein MJ, Nance RM, Delaney JAC, et al. Mortality following myocardial infarction among HIV-infected persons: the Center for AIDS Research Network Of Integrated Clinical Systems (CNICS). BMC Med 2019;17:149.
- Butt AA, Chang CC, Kuller L et al. Risk of heart failure with human immunodeficiency virus in the absence of prior diagnosis of coronary heart disease. Arch Intern Med 2011;171:737-43.
- Remick J, Georgiopoulou V, Marti C, et al. Heart failure in patients with human immunodeficiency virus infection: epidemiology, pathophysiology, treatment, and future research. Circulation 2014;129:1781-9.
- Freiberg MS, Chang CC, Kuller LH, et al. HIV infection and the risk of acute myocardial infarction. JAMA Intern Med 2013;173:614-22.
- Paisible AL, Chang CC, So-Armah KA, et al. HIV infection, cardiovascular disease risk factor profile, and risk for acute myocardial infarction. J Acquir Immune Defic Syndr 2015;68:209-16.
- Ntsekhe M, Baker JV. Cardiovascular disease among persons living with hiv: new insights into pathogenesis and clinical manifestations in a global context. Circulation 2023;147:83-100.
- Libby P, Ridker PM, Hansson GK. Progress and challenges in translating the biology of atherosclerosis. Nature 2011;473:317-25.
- Lederman MM, Calabrese L, Funderburg NT, et al. Immunologic failure despite suppressive antiretroviral therapy is related to activation and turnover of memory CD4 cells. J Infect Dis 2011;204:1217-26.
- Sereti I, Krebs SJ, Phanuphak N, et al. Persistent, Albeit reduced, chronic inflammation in persons starting antiretroviral therapy in acute HIV infection. Clin Infect Dis 2017;64:124-31.
- Neuhaus J, Jacobs DR, Jr., Baker JV, et al. Markers of inflammation, coagulation, and renal function are elevated in adults with HIV infection. J Infect Dis 2010;201:1788-95.
- Deeks SG, Tracy R, Douek DC. Systemic effects of inflammation on health during chronic HIV infection. Immunity 2013;39:633-45.
- Temu TM, Polyak SJ, Zifodya JS, et al. Endothelial dysfunction is related to monocyte activation in antiretroviral-treated people with HIV and HIV-negative adults in Kenya. Open Forum Infect Dis 2020;7:ofaa425.
- Feinstein MJ. HIV and cardiovascular disease: from insights to interventions. Top Antivir Med 2021;29:407-11.
- Feinstein MJ, Hsue PY, Benjamin LA, et al. Characteristics, prevention, and management of cardiovascular disease in people living with HIV: a scientific statement from the American Heart Association. Circulation 2019;140:e98-e124.
- El-Sadr WM, Lundgren J, et al. CD4+ count-guided interruption of antiretroviral treatment. N Engl J Med 2006;355:2283-96.
- Group DADS, Sabin CA, Worm SW, et al. Use of nucleoside reverse transcriptase inhibitors and risk of myocardial infarction in HIV-infected patients enrolled in the D:A:D study: a multi-cohort collaboration. Lancet 2008;371:1417-26.
- Panel on Antiretroviral Guidelines for Adults and Adolecents. Recommendations for the Use of Statin Therapy as Primary Prevention of Atherosclerotic Cardiovascular Disease in People with HIV. Available here.
- Grinspoon SK, Fitch KV, Zanni MV, et al. Pitavastatin to prevent cardiovascular disease in HIV infection. N Engl J Med 2023;389:687-99.
- Ridker PM, Danielson E, Fonseca FA, et al. Reduction in C-reactive protein and LDL cholesterol and cardiovascular event rates after initiation of rosuvastatin: a prospective study of the JUPITER trial. Lancet 2009;373:1175-82.
- Chastain DB, Stover KR, Riche DM. Evidence-based review of statin use in patients with HIV on antiretroviral therapy. J Clin Transl Endocrinol 2017;8:6-14.
- Panel on Antiretroviral Guidelines for Adults and Adolecents. Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents with HIV. Department of Health and Human Services. Available here.
- Eyawo O, Brockman G, Goldsmith CH, et al. Risk of myocardial infarction among people living with HIV: an updated systematic review and meta-analysis. BMJ Open 2019;9:e025874.
- Triant VA, Perez J, Regan S, et al. Cardiovascular risk prediction functions underestimate risk in HIV infection. Circulation 2018;137:2203-14.
- Sattar N, Preiss D, Murray HM, et al. Statins and risk of incident diabetes: a collaborative meta-analysis of randomised statin trials. Lancet 2010;375:735-42.
- Warden BA, Guyton JR, Kovacs AC, et al. Assessment and management of statin-associated muscle symptoms (SAMS): A clinical perspective from the National Lipid Association. J Clin Lipidol 2023;17:19-39.
Clinical Topics: Prevention
Keywords: Cardiology Magazine, ACC Publications, HIV Infections, Primary Prevention, Anti-Retroviral Agents, Chronic Disease, Integrase Inhibitors, HIV Integrase Inhibitors