
Cutting-Edge Structural Interventions | TAVR Thrombosis: Can Surgery Be Avoided?

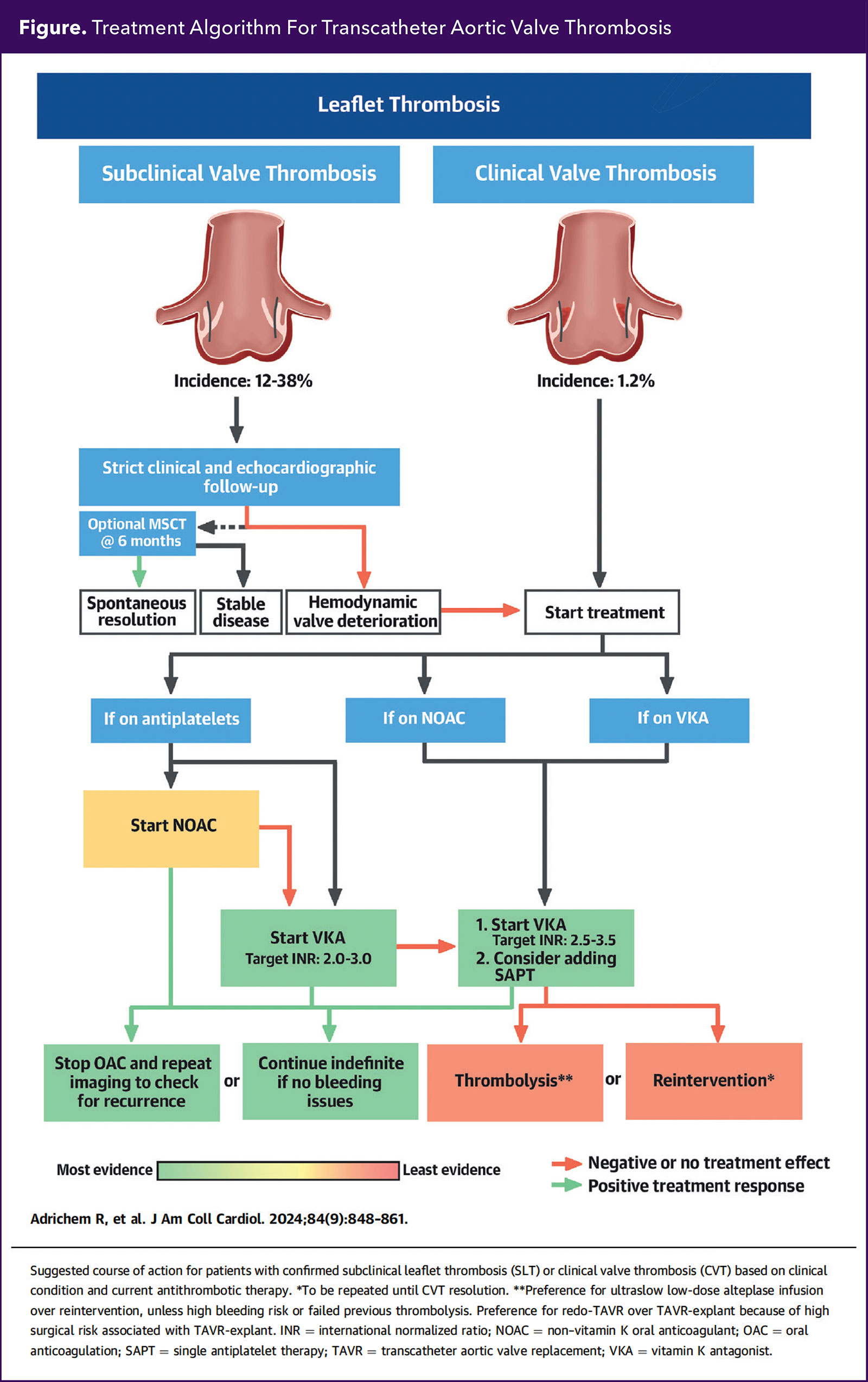
Subclinical leaflet thrombosis (SLT) has raised concerns about the long-term durability and outcomes of transcatheter aortic valve replacement (TAVR). Clinical valve thrombosis (CVT) is a rare complication after TAVR with an incidence of 0.6–2.8%.1
Treatment with oral anticoagulants (OAC) may resolve thrombosis in most of cases of SLT, and thrombolytics, surgery or repeat TAVR can be reserved for severe cases of CVT.
SLT and CVT
TAVR-related thrombosis can be divided into SLT and CVT. SLT presents as an incidental finding on follow-up cardiac CT scans and CVT presents with symptoms of heart failure (HF), aortic stenosis and high valvular gradients.
Data from landmark clinical trials have demonstrated that the incidence of SLT is high at 10-17% at 30 days in balloon-expandable valves and 17% at 30 days in self-expanding valves.2,3
SLT can present as hypo-attenuated leaflet thickening (HALT), which can be associated with reduced leaflet motion (RLM). The significance of SLT is unclear, and usually does not present with symptoms or worsening hemodynamic performance of the TAVR valve. RLM can present with higher TAVR gradients when compared with baseline.4
Data from the PARTNER trials and SURTAVI trials demonstrated that CVT has a low incidence of 0.5-2.5% in self-expanding valves and 0.5% in balloon-expandable valves respectively. CVT presentations can range from aortic stenosis, regurgitation, HF and cardiogenic shock.5,6
The pathophysiology of SLT/CVT is poorly understood but can be related to the native valve remaining in place acting as a prothrombotic substrate, and under expansion of the valve can lead to more platelet aggregation and stasis from neo-sinus creation. There is no difference in SLT rates between TAVR and bioprosthetic surgical aortic valve replacement (SAVR).7
Diagnosis
The diagnosis of SLT is incidental in follow-up CT scans. Due to poor spatial resolution transthoracic and transesophageal echocardiograms can miss HALT. The degree of HALT can be stratified according to the severity of reduced leaflet motion and the percentage of annular involvement.7
The ACC/American Heart Association valvular heart disease guideline recommends cardiac CT and/or a transesophageal echocardiogram when there is new unexplained HF, neurological symptoms and an increase in gradient to rule out leaflet thrombosis.
After diagnosis and treatment of SLT/CVT, the gradient can be followed by repeat transthoracic echocardiograms. A follow-up echocardiogram at three months is recommended to assess response to therapy. At three to six months, a follow-up CT scan is optional to monitor therapeutic response.7
Treatment of SLT
SLT may resolve spontaneously. Data have demonstrated that 35-54% of HALT cases resolved at one-year follow-up without changes in treatment. Of cases of SLT, 15% progress to RML and 3-9% of cases of HALT progress to CVT.7
Observational data have demonstrated that treatment with a novel OAC (NOAC) or a vitamin K antagonist (VKA) is superior to antiplatelet therapy alone for resolution of SLT.8
In the ATLANTIS 4D CT trial, there was evidence that the use of OAC with apixaban and VKA decreased the incidence of SLT in patients post TAVR without an OAC indication.
Clinical trials have demonstrated harm with the routine use of OAC after TAVR in the absence of an indication for anticoagulation.9,10
Due to this signal of harm with OAC, the decision to change therapy in the setting of SLT should be individualized and should be reserved for patients with more severe SLT with RLM, symptoms and higher baseline gradients.
Treatment of CVT
CVT can present with a wide clinical spectrum ranging from high aortic gradients to severe aortic stenosis with cardiogenic shock. Oral anticoagulation with a NOAC or VKA is recommended in anticoagulation-naïve patients. In patients already on a NOAC, switching to VKA with an INR 2-3 is recommended.
In patients already on a VKA, higher INR values of 2.5-3 are desired. When using VKA, we recommend a heparin bridge until the INR target is achieved.
Using this therapeutic strategy, case reports of around 131 patients have demonstrated resolution of thrombosis in 91.6% of cases based on repeat imaging or normalization of gradients.
Practice Pearls

SLT after TAVR is common and can regress spontaneously.
CVT after TAVR is uncommon and requires OAC therapy.
CCTA is highly beneficial for confirming the diagnosis of SLT and/or CVT, and for assessing and monitoring response to treatment.
Anticoagulation options can be VKA, NOAC and, less frequently, ultraslow low-dose thrombolysis.
Data are limited on appropriate treatment for TAVR thrombosis.
Surgical explant is associated with high morbidity and mortality.
There are fewer case reports concerning the use of NOACs, but normalization of gradients can be achieved at three to four months. No comparison between NOACs has been described.
Data from the Mayo Clinic registry of patients with SAVR and TAVR demonstrated recurrence of thrombosis in 23% of cases after discontinuation of NOACs or VKA with a median time for recurrence of 23 months.11
Due to the high recurrence rate, repeat cardiac CT at three to six months might be beneficial. The necessary duration of anticoagulation therapy is unclear.
In patients in whom anticoagulation fails or who have severe symptoms and are at high risk for surgery, thrombolytic agents can be recommended. Data from two clinical trials that included patients with mechanical valve thrombosis demonstrated that low-dose infusion of 25 mg of alteplase over 25 hours had a 90% success rate with a low complication risk.12,13
Data from a nonrandomized study demonstrated that low-dose tissue plasminogen activator (t-PA) use in mechanical valve thrombosis was associated with a success rate of about 90% and lower three-month mortality and complications when compared with surgery.14
The use of thrombolytics in bioprosthetic valves and TAVR valves has not been well established, with only a small number of case reports suggesting thrombus resolution at low risk.7
The ACC/AHA valvular heart disease guideline recommends urgent treatment with low-dose thrombolytics or emergent surgery in left-sided mechanical prosthetic valve obstruction with symptoms.
In patients with suspected or confirmed bioprosthetic valve thrombosis who are stable and do not have a contraindication for anticoagulation, initial treatment with VKA might be reasonable. There are no recommendations for the role of NOACs, fibrinolytics or surgery in this setting.
There are limited data about reintervention (valve-in-valve [ViV] TAVR or TAVR explant surgery). The EXPLANT TAVR registry demonstrated that explant surgery is a high-risk procedure with a mortality of 13% at 30 days.15
ViV TAVR can be safe and often becomes the strategy of choice in patients with high or prohibitive surgical risk. Distal embolic protection should be considered when possible to mitigate the potential risk of distal embolization of thrombotic debris.
Our Practice Approach
In the presence of SLT with hemodynamic valve deterioration, severe SLT with RLM or CVT, we recommend starting OAC with a NOAC or VKA. If the patient is already on OAC, we recommend changing to VKA with higher INR levels of 2.5-3.5 and considering adding single antiplatelet therapy.
OAC is to be continued lifelong if no bleeding issues are present or after improvement of gradients by echocardiography and SLT severity by cardiac CT scan. If there is no improvement, we recommend a trial of thrombolytics with an ultraslow-dose infusion of 25 mg of alteplase and then continued OAC with VKA with INR levels of 2.5-3.5.
If improvement is still not seen, and only in very severe cases of SLT with RLM or CVT, surgical explanation should be considered with its high mortality risk.7


References
- Otto CM, Nishimura RA, Bonow RO, et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: Executive Summary. Circulation 2021;143:e35-e71.
- Sibilitz KL, Fukutomi M, Sondergaard L. Valve thrombosis after transcatheter aortic valve replacement-cause for concern? Ann Cardiothorac Surg 2020;6:505-7.
- Makkar RR, Blanke P, Leipsic J, et al. Subclinical leaflet thrombosis in transcatheter and surgical bioprosthetic valves: PARTNER 3 cardiac computed tomography substudy. J Am Coll Cardiol 2020;75:3003-15.
- Blanke P, Leipsic JA, Popma JJ, et al. Bioprosthetic aortic valve leaflet thickening in the Evolut low risk sub-study. J Am Coll Cardiol 2020;75:2430-42.
- Chakravarty T, Søndergaard L, Friedman J, et al. Subclinical leaflet thrombosis in surgical and transcatheter bioprosthetic aortic valves: an observational study. Lancet 2017;389:2383-92.
- Mack MJ, Leon MB, Thourani VH, et al. Transcatheter aortic-valve replacement in low-risk patients at five years. N Engl J Med 2023;389:1949-60.
- Forrest JK, Deeb GM, Yakubov SJ, et al. 4-Year outcomes of patients with aortic stenosis in the Evolut Low Risk Trial. J Am Coll Cardiol 2023;82:2163-2165.
- Adrichem R, Rodes Cabau J, Mehran R, et al. Treatment of transcatheter aortic valve thrombosis: JACC review topic of the week. J Am Coll Cardiol 2024;84:848-61.
- Holy EW, Kebernik J, Allali A, et al. Comparison of dual antiplatelet therapy versus oral anticoagulation following transcatheter aortic valve replacement: A retrospective single-center registry analysis. Cardiol J 2017;24:649-59.
- Montalescot G, Redheuil A, Vincent F, et al. Apixaban and valve thrombosis after transcatheter aortic valve replacement: The ATLANTIS-4D-CT Randomized clinical trial substudy. JACC Cardiovasc Interv 2022;15:1794-1804.
- Dangas GD, Tijssen JGP, Wöhrle J, et al. A controlled trial of rivaroxaban after transcatheter aortic-valve replacement. N Engl J Med 2020;382:120-9.
- Petrescu I, Egbe AC, Ionescu F, et al. Long-term outcomes of anticoagulation for bioprosthetic valve thrombosis. J Am Coll Cardiol 2020;75:857-66.
- Özkan M, Gündüz S, Biteker M, et al. Comparison of different TEE-guided thrombolytic regimens for prosthetic valve thrombosis: the TROIA trial. JACC Cardiovasc Imaging 2013;6:206-16.
- Özkan M, Gündüz S, Gürsoy OM, et al. Ultraslow thrombolytic therapy: A novel strategy in the management of PROsthetic MEchanical valve Thrombosis and the prEdictors of outcomE: The Ultra-slow PROMETEE trial. Am Heart J 2015;170:409-18.
- Özkan M, Gündüz S, Güner A, et al. Thrombolysis or Surgery in patients with obstructive mechanical valve thrombosis: The Multicenter HATTUSHA study. J Am Coll Cardiol 2022;79:977-89.
- Bapat VN, Zaid S, Fukuhara S, et al. Surgical explantation after TAVR failure: Mid-term outcomes from the EXPLANT-TAVR international registry. JACC Cardiovasc Interv 2021;14:1978-91.
Clinical Topics: Cardiac Surgery, Cardiovascular Care Team, Invasive Cardiovascular Angiography and Intervention, Valvular Heart Disease, Cardiac Surgery and VHD, Interventions and Structural Heart Disease
Keywords: Cardiology Magazine, ACC Publications, Transcatheter Aortic Valve Replacement, Heart Valve Diseases