From the Member Sections | The Primary Palliative Care We Already Provide: Supportive Care For CV Patients

You care for a 75-year-old woman with heart failure (HF) with reduced ejection fraction. For the years you have known her, she has enjoyed spending time with her grandchildren, living independently and being an active member of her community.
But in the past year, her ability to pursue these activities has declined, limited by worsening edema, dyspnea, fatigue, pain and low mood. She has been hospitalized twice for HF exacerbations and has developed diuretic resistance. She has lost muscle mass and appears more frail. She says, "I don't know, Doc. I'm getting tired of all of this."
Addressing the symptom burden experienced by patients with HF can be challenging. Yet, it is the foundation of what we do in cardiovascular care. By systematically identifying life-limiting symptoms, we hone in on how to best help our patients, calling on the primary palliative care skills we use every day.
Providing Primary Palliative Care as a CV Clinician
Palliative care improves quality of life, reduces depression and anxiety, improves patients' prognostic understanding, and increases the likelihood that the care patients receive is in line with their goals and values. Primary palliative care is delivered by the main team caring for patients with a serious illness, such as the cardiovascular team.
The ACC/AHA/HFSA Guideline on Heart Failure recommends clinicians employ primary palliative care skills to communicate prognosis, elicit patients' values and engage in shared decision-making to clarify goals of care, manage cardiovascular-related symptoms and support caregivers.1
Many of our patients may benefit from palliative care, whether their symptoms are due to HF, chronic ischemia, valvular disease, peripheral vascular disease, pulmonary hypertension or congenital heart disease. As cardiovascular clinicians, we already provide primary palliative care to our patients by managing symptoms, engaging in shared decision-making and advance care planning.
Importantly, we must know when to refer patients to specialist palliative care or hospice when needed. Our patients and their families trust us to have these conversations, and while challenging at times, we're equipped to do so.
We're adept at performing comprehensive symptom management and offering solutions that provide relief. A thorough assessment for angina, hypervolemia and exercise tolerance are focal points for any cardiac review of symptoms.
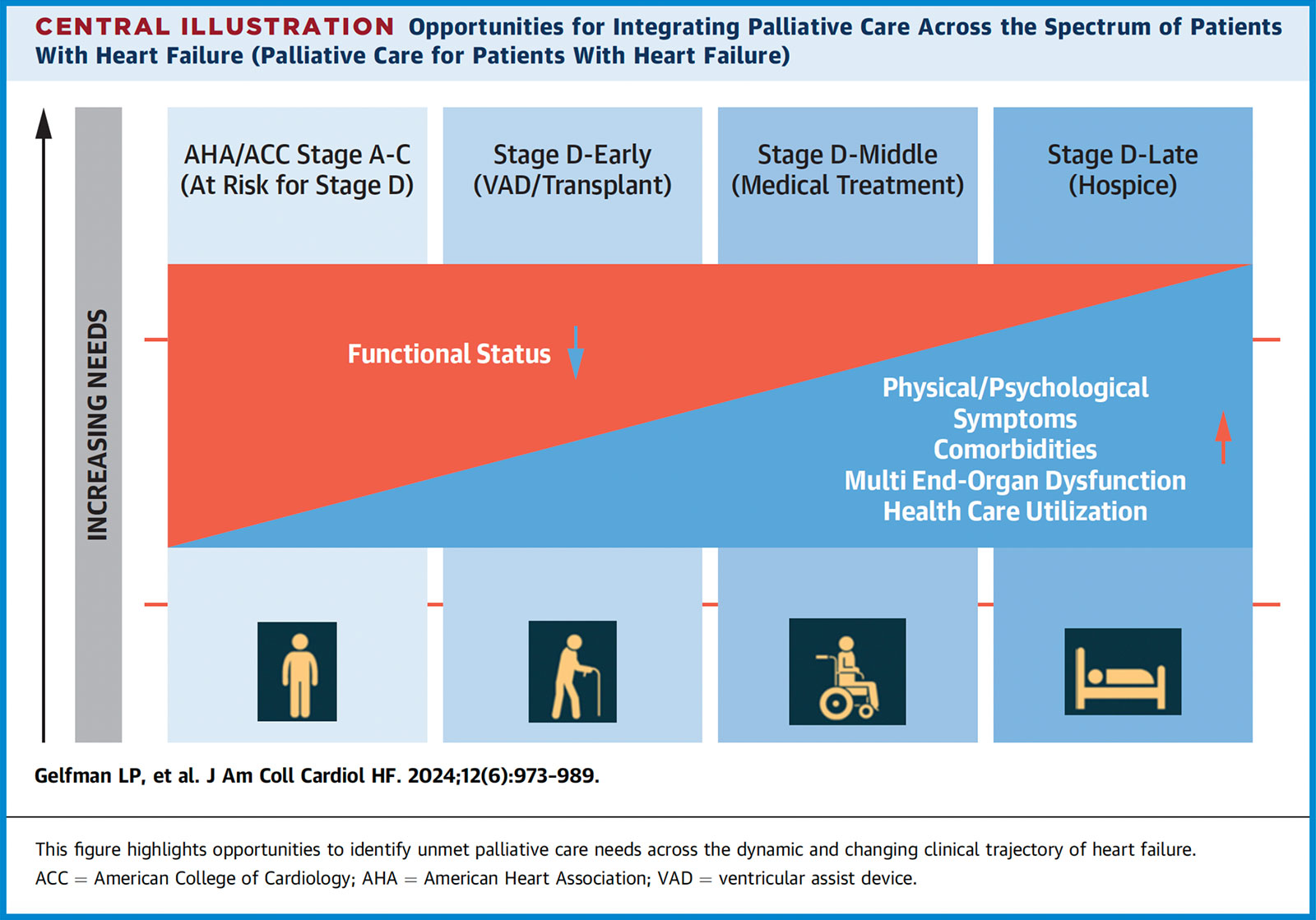
We have a large armamentarium of medications that we commonly prescribe for symptom relief, including guideline-directed medical therapy for HF and coronary artery disease, diuretics and antianginal drugs. Opportunities for integrating palliative care for patients with HF are outlined above (Figure).
Some of us manage advanced HF patients on palliative inotropes; this requires in-depth shared decision-making and evaluation for support at home, which are cornerstones to supportive care. Aerobic exercise, for which we can provide a prescription or refer to physical therapy, improves fatigue, dyspnea and well-being in people with HF. Many devices and therapeutics also relieve symptoms, like coronary interventions, cardiac resynchronization, and valve repair or replacement.
We're also well-equipped to assess for and treat anxiety and depression and to refer to mental health specialists when patients' needs exceed our capabilities.
A CV Clinician's Role in Advance Care Planning

As we guide patients through their HF course, advance care planning (ACP) should be included. ACP is the process of preparing for decisions about future medical care by anticipating significant health events or changes in functional status, addressing "what-ifs." By helping patients think through their wishes, ACP can improve patients' quality of life and sense of control.
ACP is especially important for people who do not want aggressive treatments, but it's not meant to dissuade patients from pursuing further care. Cardiovascular clinicians have the benefit of long-term relationships with patients that give us many opportunities to engage in these conversations.
ACP begins with education about expected disease progression and treatment options. Through discussion, we may elicit a patient's values and priorities and make plans for when they are seriously ill or unable to communicate. Identification of a surrogate decision-maker is a key part of ACP, as patients may prefer someone other than their legal next of kin.
Related Resources
Click here for ACC's self-paced, free online on-demand course, Palliative Care for the Cardiovascular Clinician, geared to help cardiologists gain skills in these areas.
Click here for the 2024 ACC ECDP on Clinical Assessment, Management, and Trajectory of Patients Hospitalized With Heart Failure for guidance on involving specialty palliative care.
Click here to access resources from CardioSmart to facilitate shared decision-making conversations.
Discussing code status as part of ACP can be a critical intervention to help patients anticipate what kind of life-sustaining interventions would be consistent with their goals.
Changes in a patient's functional status can present a meaningful opportunity to revisit ACP conversations. Patients' concerns and wishes are likely to change as their disease progresses, so ACP discussions and documents should be re-visited and updated as needed over time.
Aside from identifying a surrogate decision-maker, eliciting information about a patient's caregiver support is a crucial component of primary palliative care. Identifying caregivers and what they need to successfully accomplish this role is essential to implementing care plans.
When these details are elicited, clinicians can refer caregivers to social workers who can, for example, connect them to community resources, arrange home-based services or assist with medical leave.
Partnering With Specialty Palliative Care Clinicians
When patients face symptoms or challenges beyond the scope of primary palliative care, we should refer them to specialty palliative care, provided by an interprofessional team.
Cardiovascular clinicians should partner with palliative care clinicians to guide management of medications, avoiding particularly deleterious medications. In particular, NSAIDs and gabapentin should be avoided given their effects on fluid retention and renal metabolism.
Morphine and codeine should be avoided in renal dysfunction due to the accumulation of active metabolites. Palliative care clinicians can prescribe other opioids or other agents to help manage pain or dyspnea as well as tools for managing cachexia and depression.
In addition to managing physical symptoms, an array of nonmedication interventions may be used to address patient and family spiritual or psychosocial concerns.
Device Deactivation: Complex Decision-Making

While ICDs can be lifesaving in preventing sudden cardiac death, they can also cause physical pain and emotional distress, particularly for patients who are approaching end of life. Up to one-third of patients are shocked in the last 24 hours of life, regardless of code status or hospice enrollment.2,3
To ensure our patients' ICD settings are aligned with their goals of care, we should advise patients on the option of deactivation at the time of implant and whenever the clinical trajectory or goals of care change. ICD deactivation decisions usually fall within the domain of primary palliative care, provided by either the primary cardiologist or electrophysiologist.
Deactivation of other cardiac devices raise more ethical concerns that may benefit from a multidisciplinary team discussion involving cardiology and specialty palliative care. For example, some believe the deactivation of a permanent pacemaker (PPM) is akin to physician-assisted death, particularly if a patient is pacemaker-dependent.
Pacemaker deactivation is rare, as there are few associated symptoms or side effects that might prompt a patient to request it. To guide these challenging conversations, the Heart Rhythm Society outlined ethical practice guidelines for deactivation of PPMs.4
Left ventricular assist device (LVAD) deactivation is more common but remains challenging to manage. Patients dying from LVAD complications (e.g., hemorrhagic stroke) or noncardiac causes (e.g., end-stage cancer) may wish to have their LVAD deactivated.
This decision can be fraught for patients, loved ones and medical team members alike, as LVADs are a frank form of life support. In these cases, involvement of specialty palliative care can be essential to provide additional patient and family support as well as to address severe symptoms and death that may follow deactivation.
When to Consider Hospice

Hospice may be a suitable end-of-life care option for patients with advanced cardiovascular disease. Hospice is an insurance benefit and care delivery model that specifically focuses on symptom control and comfort.
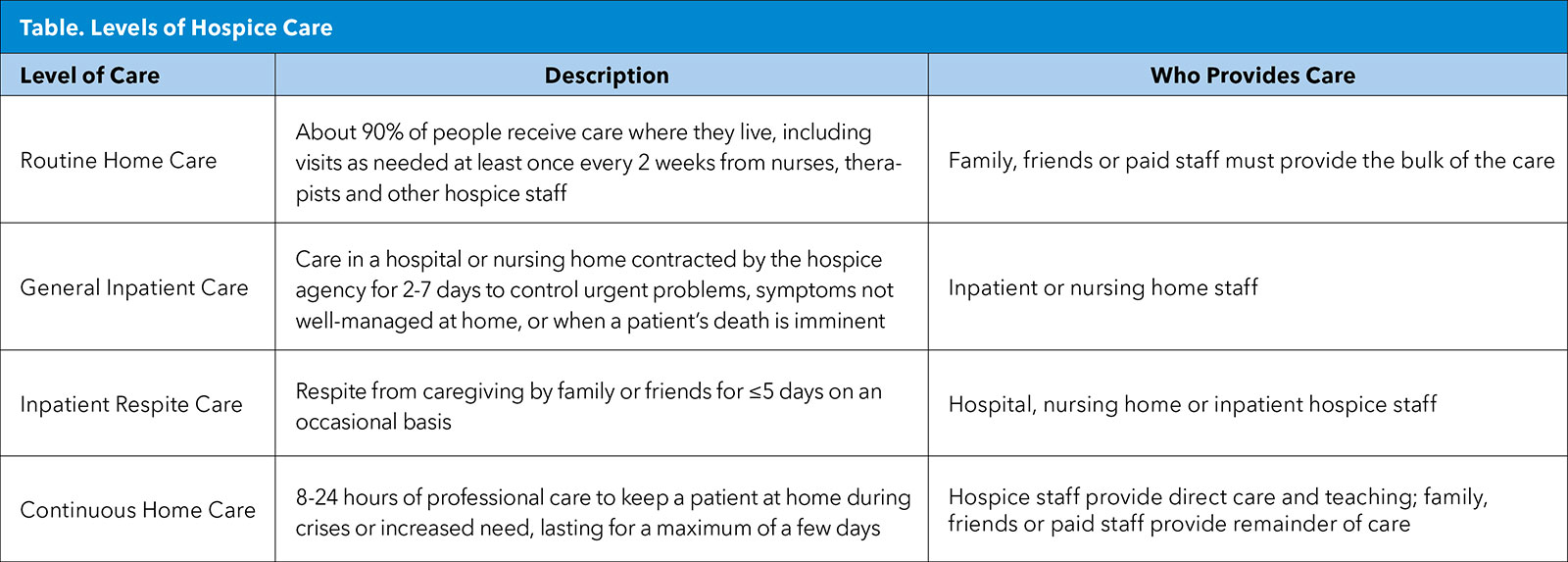
It is provided to patients with an estimated prognosis of six months or less and is a helpful intervention when rehospitalization is undesirable or if discharge home is desired despite significant medical needs. Hospice comprises four levels of care as described below (Table).
With a growing body of evidence on how primary and specialty palliative care meaningfully improves patients' quality of life, symptoms and overall well-being throughout the HF trajectory, we are fortunate that we have more pharmacologic, interdisciplinary and psychosocial tools to deliver truly patient-centered care across the continuum of cardiovascular care.
This article was authored by Ramya Sampath, MD, internal medicine resident, Yale New Haven Hospital; Jadry Gruen, MD, cardiovascular medicine fellow, Hospital of the University of Pennsylvania; Jill M. Steiner, MD, MS, FACC, assistant professor, Division of Cardiology, University of Washington; Sarah Godfrey, MD, MPH, cardiology and palliative care fellow, University of Texas Southwestern Medical Center; Sarah J. Goodlin, MD, medical director, Geriatrics and Palliative Care Medicine, VA Portland Health System; and Jill M. Patton, CRNP, AACC, acute care nurse practitioner, Section of Palliative Medicine, Johns Hopkins Hospital. All are members of ACC's Geriatric Cardiology Member Section.
Click here to learn more about joining this and other Sections.
References
- Heidenreich PA, Bozkurt B, Aguilar D, et al. 2022 AHA/ACC/HFSA guideline for the management of heart failure. J Am Coll Cardiol 2022;79:e263-e421.
- Kinch Westerdahl A, Sjöblom J, Mattiasson AC, Rosenqvist M, Frykman V. Implantable cardioverter-defibrillator therapy before death: high risk for painful shocks at end of life. Circulation 2014;129:422-9.
- Mitchell LB, Pineda EA, Titus JL, Bartosch PM, Benditt DG. Sudden death in patients with implantable cardioverter defibrillators: the importance of post-shock electromechanical dissociation. J Am Coll Cardiol 2002;39:1323-8.
- Lampert R, Hayes DL, Annas GJ, et al. HRS Expert Consensus Statement on the Management of Cardiovascular Implantable Electronic Devices (CIEDs) in patients nearing end of life or requesting withdrawal of therapy. Heart Rhythm 2010;7:1008-26.
Clinical Topics: Cardiovascular Care Team
Keywords: Cardiology Magazine, ACC Publications, Palliative Care, Quality of Life, Patient Care Planning, Advance Care Planning, Hospices