
From the Member Sections | The Evolution of Practice in Structural Disease/Valve Treatment: A Triumph of Collaboration

The first successful percutaneous transluminal coronary angioplasty was performed by Andreas Gruentzig, MD, in September 1977. Despite careful lesion selection, the initial equipment consisted of crude guiding catheters that were difficult to maneuver and non-over-the-wire balloon catheters with a leading short, shapeable wire tip.
The challenges created by equipment limitations plus the recognition that balloon-dilated lesions could acutely occlude (there were no stents) and lead to myocardial infarction or hemodynamic collapse led to a need for backup by cardiothoracic surgeons (CTS) for emergency bypass surgery.
The continued collaboration between interventional cardiologists (IC) and CTS led to the formation of heart teams that work closely to make treatment decisions for patients with complex coronary disease.
With the success of heart teams in the coronary space, the collaboration evolved further into heart teams in structural heart disease (SHD) where IC and CTS along with other specialists work together to formulate treatment plans for patients with SHD.1
Here we discuss the collaborative work of IC and CTS in treating patients with SHD in various settings ranging from preprocedure evaluation and formulating treatment plans to performing procedures as a team along with postprocedure care.
Preprocedure Workup For SHD Patients
Learn More at ACC.25
Don't miss the following TAVR-related sessions and more at ACC.25 in Chicago from March 29-31.
Click here for the Online Planner and explore sessions like The Mitral Movement (#244), The Future of TAVR (#377) and the Joint ACC/STS Symposium on Emerging Challenges in Post-TAVR Cardiac Surgery (#330).
The multidisciplinary Heart Valve Team (HVT) concept in SHD originated with the pivotal clinical trials comparing TAVR and SAVR in aortic stenosis (AS).2 The surgeons served as the arbiters of the level of risk (high, intermediate, low) in the respective trials.3
Consequently, the Centers for Medicare and Medicaid Services (CMS) mandated joint participation by IC and CTS in TAVR.4 With approval by the U.S. Food and Drug Administration of TAVR in patients with low surgical risk, the appraisal of surgical risk as an isolated assessment is moot and the role of the HVT has evolved.
In addition to IC and CTS, the modern HVT comprises structural imaging specialists, clinical cardiologists, cardiac anesthesiologists and valve care coordinators.
Treatment evaluation for TAVR or SAVR includes assessment of concomitant cardiac pathology, anatomical risk for TAVR or SAVR, socioeconomic factors, patient values and preferences.
Besides achieving optimal outcomes with the index therapy, HVT evaluation and shared-decision making discussions have evolved to lifetime management options and the feasibility of future valve-in-valve TAVR or redo-TAVR.
In mitral and tricuspid valve disease, with the advent of both transcatheter repair and replacement options, the decision-making process is even more complex than for AS treatment.
Specifically for secondary mitral regurgitation (MR) or tricuspid regurgitation (TR), the participation of heart failure specialists as part of the HVT evaluation is crucial, as was mandated by pivotal trials of transcatheter MR and TR technologies.5,6
Clinical practice guidelines in both the U.S. and Europe give a class I recommendation for HVT evaluation in patients with severe valvular heart disease.7,8
However, practical implementation of the HVT varies across institutions and requires added time and certain inefficiencies. Optimally, HVT evaluation should include joint clinics where patients and their families meet face-to-face with the IC, CTS and other HVT members as a team.
Depending upon individual sites, the IC and CTS may have particular expertise in aortic or mitral/tricuspid therapies and patients will likely be best served by having shared decision-making conversations with operators with specific expertise in their valve condition.
A surgeon with aortic expertise for example might not be best suited for shared decision-making conversations around mitral valve repair or replacement in primary MR.
Following clinic assessments, multidisciplinary meetings have also become common ground and bring multiple specialists from cardiology and cardiac surgery divisions together to discuss therapeutic recommendations and preferred treatment strategy.
These multidisciplinary meetings are conducted in-person or in virtual formats depending on institutional preference. In busy structural programs, these have evolved to separate aortic- or mitral/tricuspid-specific meetings.
Regular and well planned HVT meetings are the backbone for SHD programs and allow for appropriate patient, procedure and equipment selection leading to smooth performance of these complex procedures and good outcomes.
Collaboration For Structural Heart Procedures
Teaming Up To Make History
The ACC and The Society of Thoracic Surgeons played a leading role in the evolution of TAVR in the U.S., working from the very beginning with the FDA, CMS and industry. "The Heart Team approach to TAVR embraced collaboration from the original trial design to active procedure performance together to rational dispersion of the new procedure and generation of real-world evidence," wrote David R. Holmes Jr, MD, MACC, and Michael J. Mack, MD, MACC, in a Cardiology article celebrating the 20th Anniversary of TAVR in 2022.
Click here for their story.
The partnership between IC and CTS is critical in the procedure suite as they jointly perform transcatheter structural heart procedures. The proficiency of the IC in wire and catheter techniques and the deep understanding of the CTS of the heart's 3D structures are complimentary and essential for the success of these complex procedures.
The IC and CTS also collaborate with other key multidisciplinary team members, including cardiac imaging specialists with expertise in interventional imaging and cardiovascular anesthesiologists, during these procedures.
Planning for these procedures begins during heart team meetings, where the team identifies suitable patients, access site and equipment while anticipating potential challenges and formulating strategies to address them.
Although procedural complications have decreased significantly as IC and CTS gain more experience, emergencies requiring open-heart surgery may occur. The presence of a CTS during the procedure enables immediate surgical intervention, minimizing delays and potentially saving lives.
However, such surgeries carry a high mortality risk of around 50%, and decisions in these situations must be made quickly through collaborative discussions between the operators.
While CMS mandates that TAVR be performed by both an IC and a CTS, mitral valve repair may be performed by either an IC or CTS or both.9 Other procedures that are also performed by both IC and CTS and currently in the trial phase include transcatheter mitral valve replacement (TMVR) and transcatheter tricuspid valve replacement (TTVR).
Training is a vital component for mastering these advanced structural procedures, whether a dedicated interventional structural fellowship,10,11 or learning on the job under the mentorship of experienced operators.
Some CTS are also opting for an additional year of interventional structural training in the catheterization lab to enhance their expertise. Both IC and CTS play active roles in training future generations of specialists and catheterization lab staff to perform these highly complex procedures.
It's well established that higher procedural volumes correlate with better outcomes,12,13 making it essential for both IC and CTS to maintain case volumes in their respective fields.
The success of any program is tied to quality and the centers performing structural heart procedures are required to participate in national registries like the STS/ACC TVT Registry as mandated by CMS.4,9
The national outcomes from the registry provide benchmarks for structural heart programs, allowing them to regularly modify their own processes and continually improve outcomes. Thus, the care of the SHD patient continues beyond the procedure suite to postprocedure care.
Postprocedural Management of SHD Patients
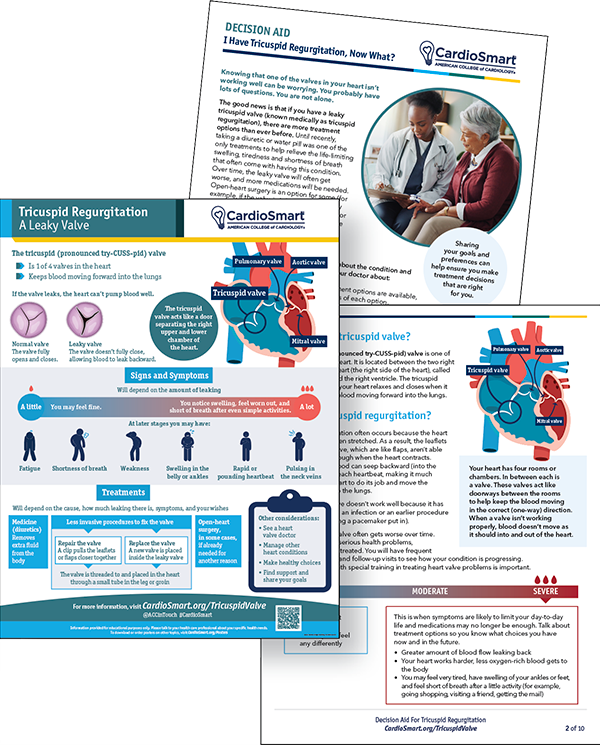
Tricuspid Regurgitation Hub
Visit CardioSmart.org/TricuspidValve to download these free new tools to support shared decision-making conversations with patients. Be sure to look for the poster-size version of the infographic packaged with this issue.
Postprocedural management following any surgical or transcatheter structural intervention includes optimization of guideline-directed medical therapy (GDMT), anticoagulation, endocarditis prophylaxis, clinical and imaging follow-up, and physical rehabilitation. These require a multidisciplinary collaborative effort.
As stated in the ACC/American Heart Association (AHA) Guideline for the Management of Patients With Valvular Heart Disease, any valve intervention replaces native disease with other challenges, including early postprocedural complications, management of other concurrent cardiac conditions, and long-term sequalae.7
Notably, clinical symptoms do not consistently herald bioprosthetic valve dysfunction or degeneration. As such, advanced imaging is necessary to identify and grade paravalvular leak, hypoattenuated leaflet thickening (HALT) with restricted mobility, and thrombosis.
Although HALT leads to an increase in valve gradients, there is no evidence indicating that it translates into clinical events or more rapid valve degeneration.
In a large real-world series, Santiago Garcia, MD, FACC, and colleagues noted that the incidence of HALT was 12% and it was an independent predictor of long-term mortality.14
The management of HALT is difficult and often entails oral anticoagulation with follow-up echocardiography and cardiac computed tomography. The data on anticoagulation and antiplatelets generally do not support the routine use of direct factor Xa inhibitors following transcatheter therapies. For those with underlying atrial fibrillation, close observation for bleeding and thrombotic events is a cornerstone for such high-risk individuals.
Similarly, endocarditis is a complex clinical challenge that not only requires input from infectious disease experts on the choice and duration of antibiotics, but a comprehensive strategy on the timing and type of surgical repair.
This multidisciplinary input becomes particularly important for those who develop complications such as heart block or abscesses.15
In addition to a surgeon and infectious disease expert, teams often involve microbiologists, neurologists, nephrologists, cardiologists and others as different complications arise.
Once again, the latest European Society of Cardiology (ESC) guideline emphasizes a heart team discussion and shared decision-making with patient centered goals, citing several observational studies.15
Finally, continued optimization of GDMT with monitoring of blood pressure and renal function is key to improvement in survival rates and reduction in rehospitalizations. Recent data from the COAPT trial noted a high level of intolerance prohibiting the use of all pillars of heart failure therapies or achieving target doses.16
Outpatient clinics are, therefore, crucial in order to identify adverse events and tailor the medical regimen to the individual patient.
In addition, rehabilitation postprocedure has been associated with improvement in both quality of life and outcomes following both surgical and transcatheter interventions, albeit fewer patients are referred following transcatheter valve repair or replacement procedures.17,18
The Value of Teams
The treatment of SHD has evolved significantly over the past two decades with the development of TAVR and other percutaneous valvular interventions, including mitral and tricuspid interventions.
IC and CTS, along with cardiologists, heart failure specialists, cardiac imagers, anesthesiologists and other specialists, play a crucial role in the preprocedure selection of patients, procedural technique and equipment to achieve the best outcomes.
Appropriate postprocedure care including GDMT, postoperative imaging and follow-up, cardiac rehabilitation, and participation in SHD registries all contribute to optimizing outcomes and ongoing quality improvement.
The HVT is recognized with a class I indication for the treatment of these complex patients by the ACC/AHA and ESC guidelines for management of valvular heart disease.7,19 The CMS mandates the presence of both IC and CTS for a TAVR procedure and either an IC or CTS or both for a MitraClip procedure.
As the breadth of transcatheter SHD procedures continues to increase, the HVT is branching out farther to focus on aortic and mitral/tricuspid procedures and the ongoing clinical trials of TMVR and TTVR will further increase these collaborations.
This article was authored by Poonam Velagapudi, MD, MS, FACC; Alison F. Ward, MD, FACC; S. Chris Malaisrie, MD, FACC; George Vetrovec, MD, MACC; Mirvat Alasnag, MD, FACC; and Tanush Gupta, MD, FACC, on behalf of ACC's Interventional Member Section and Cardiac Surgery Member Sections.
Click here to learn about and join this Member Section and more.
References
- Otto CM, Nishimura RA, Bonow RO, et al. 2020 ACC/AHA guideline for the management of patients with valvular heart disease. J Am Coll Cardiol 2021;143:e72-e227.
- Cribier A. Invention and uptake of TAVI over the first 20 years. Nat Rev Cardiol 2022; 19:427-8.
- Al-Azizi K, Hamandi M, Mack M. Clinical trials of transcatheter aortic valve replacement. Heart 2019;105(Suppl 2):s6-s9.
- National Coverage Determination (NCD). Transcatheter Aortic Valve Replacement (TAVR). Accessed Oct. 17 2024. Available here.
- Stone GW, Lindenfeld J, Abraham WT, et al. Transcatheter mitral-valve repair in patients with heart failure. N Engl J Med 2018;379:2307-18.
- Sorajja P, Whisenant B, Hamid N, et al. Transcatheter repair for patients with tricuspid regurgitation. N Engl J Med 2023;388:1833-42.
- Otto CM, Nishimura RA, Bonow RO, et al. 2020 ACC/AHA guideline for the management of patients with valvular heart disease. J Am Coll Cardiol 2021;143:e72-e227.
- Prendergast B, Vahanian A. The 2021 ESC/EACTS guidelines for the management of valvular heart disease: a new template for Heart Teams and their patients. Cardiovasc Res 2022;118:e11-e13.
- National Coverage Determination (NCD). Transcatheter Mitral Valve Repair (TMVR). Accessed Oct. 24, 2024. Available here.
- ACC Structural Heart Disease and Congenital Interventional Fellowship Programs. Accessed Oct. 24 , 2024. Available here.
- Bass TA, Abbott JD, Mahmud E, et al. 2023 ACC/AHA/SCAI advanced training statement on interventional cardiology (coronary, peripheral vascular, and structural heart interventions): A report of the ACC Competency Management Committee. J Am Coll Cardiol 2023;81:1386-1438.
- Vemulapalli S, Carroll JD, Mack MJ, et al. Procedural volume and outcomes for transcatheter aortic-valve replacement. N Engl J Med 2019;380:2541-50.
- Chhatriwalla AK, Vemulapalli S, Szerlip M, et al. Operator experience and outcomes of transcatheter mitral valve repair in the United States. J Am Coll Cardiol 2019;74:2955-65.
- Garcia S, Fukui M, Dworak MW, et al. Clinical impact of hypoattenuating leaflet thickening after transcatheter aortic valve replacement. Circ Cardiovasc Interv 2022;15:e011480.
- Delgado V, et al. 2023 ESC guidelines for the management of endocarditis. Eur Heart J 2023;44:3948-4042.
- Cox ZL, Zalawadiya SK, Simonato M, et al. Guideline-directed medical therapy tolerability in patients with heart failure and mitral regurgitation: The COAPT Trial. JACC Heart Fail 2023;11:791-805.
- Ribeiro GS, Melo RD, Deresz LF, et al. Cardiac rehabilitation programme after transcatheter aortic valve implantation versus surgical aortic valve replacement: Systematic review and meta-analysis. Eur J Prev Cardiol 2017;24:688-97.
- Imran HM, Baig M, Mujib M, et al. Comparison of phase 2 cardiac rehabilitation outcomes between patients after transcatheter versus surgical aortic valve replacement. Eur J Prev Cardiol 2018;25:1577-84.
- Vahanian A, Beyersdorf F, Praz F, et al. 2021 ESC/EACTS guidelines for the management of valvular heart disease. Eur Heart J 2022;43:561-632.
Clinical Topics: Cardiac Surgery, Cardiovascular Care Team, Invasive Cardiovascular Angiography and Intervention, Valvular Heart Disease, Cardiac Surgery and VHD, Interventions and Structural Heart Disease
Keywords: Cardiology Magazine, ACC Publications, Tricuspid Valve Insufficiency, Transcatheter Aortic Valve Replacement, Heart Valve Diseases, Tricuspid Valve