Cover Story | Pulmonary Hypertension: Bridging the Gap Between Recognition and Treatment
Despite affecting approximately 1% of the population and carrying significant mortality risk, pulmonary hypertension (PH) remains underrecognized compared to other cardiovascular conditions. Several interconnected factors contribute to this clinical blind spot.
But with a new drug for pulmonary arterial hypertension (PAH) and with the prevalence of PH associated with left heart disease (PH-LHD) increasing as the population ages, it's time to breathe new life into improving recognition of PH and better prepare cardiologists to manage or co-manage these patients.
PH Diagnosis Delayed or Missed
Many PH patients endure months or years of progressive symptoms before receiving an accurate diagnosis, time during which irreversible pulmonary vascular remodeling may advance unchecked. There are several reasons for this delay.
For starters, PH patients can present with nonspecific symptoms that are misdiagnosed or ignored. They then often navigate between general cardiology and pulmonology before reaching PH-specialty care, further delaying recognition and treatment. "Because neither specialty really has true ownership of the disease, patients can fall through the cracks," says Estefania Oliveros, MD, MSc, FACC, an advanced heart failure and transplant cardiology (AHFTC) specialist who focuses on PH at Columbia University Irving Medical Center in New York.
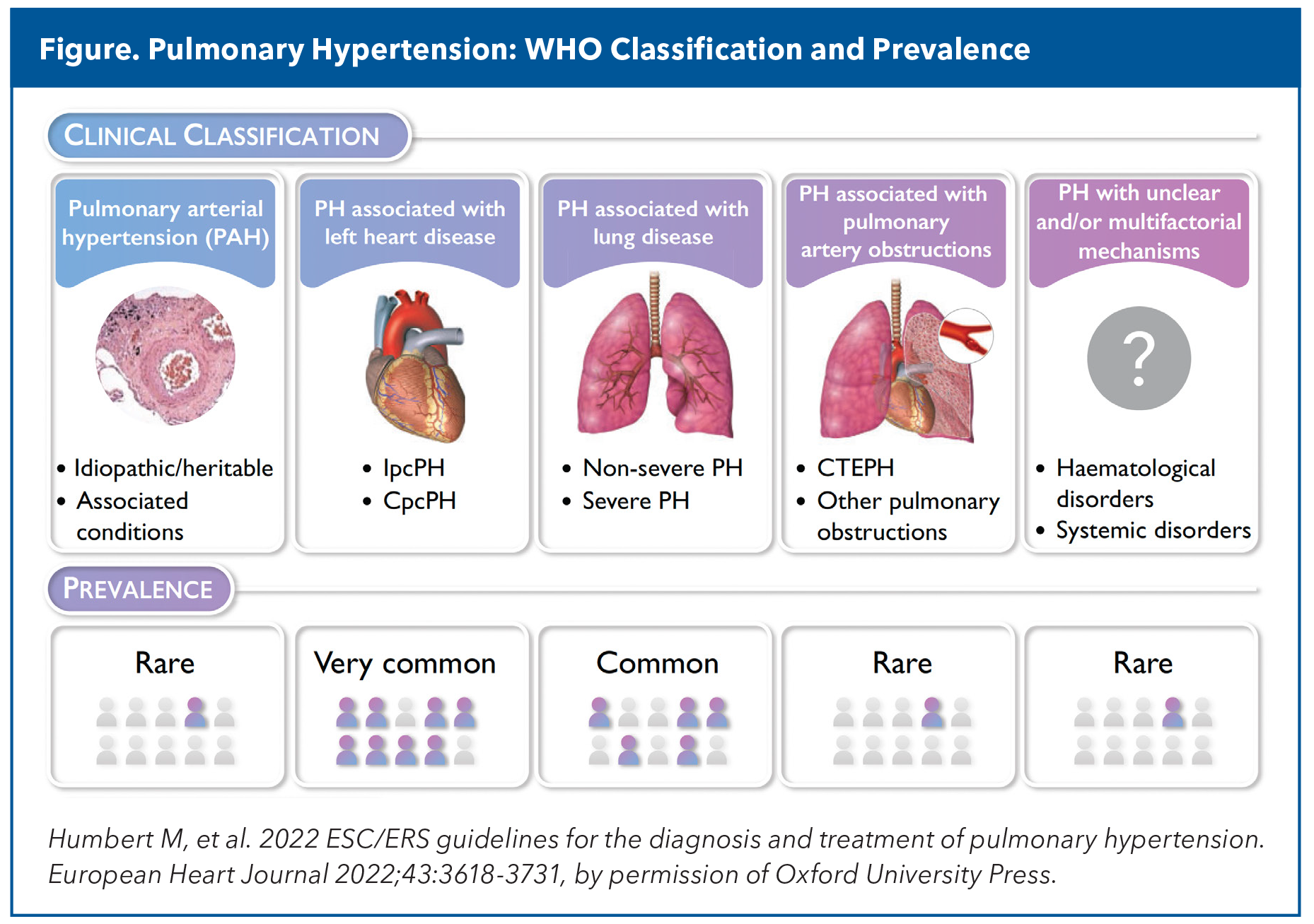
Also, cardiovascular medical training historically and persistently emphasizes left-sided cardiac disease, and most physicians feel uncomfortable interpreting right heart hemodynamics. To boot, the complex five-group WHO classification system (Figure) and specialized treatment algorithms can seem daunting to nonspecialists. And that's before thinking about the complexities of diagnosis and prescribing the specialty medications used to treat PH, of which there are 16 approved by the U.S. Food and Drug Administration (FDA).
With all this, it's not uncommon to see patients not referred to a HF specialist or PH center of excellence until they are in HF.
PAH: The Rare But Visible
PAH, or Group 1 PH, is an uncommon yet progressive disease. It affects 25 individuals per 1 million in Western countries, with an annual incidence of two to five cases per million. PAH is characterized by marked narrowing and stiffening of the pulmonary vascular bed and a progressive rise in the pulmonary vascular load, leading to hypertrophy and remodeling of the right ventricle.
Despite some advances, and with more than a dozen FDA-approved medications in several major categories (endothelin receptor antagonists, soluble guanylate cyclase stimulators, phosphodiesterase inhibitors, prostacyclins analogs/agonist, and the newer activin signaling inhibitors) that enhance exercise capacity, improve quality of life and slow disease progression, PAH still carries significant disease-associated morbidity and mortality.
While all forms of PH face recognition challenges, PAH confronts perhaps the greatest diagnostic hurdles, says Oliveros. Unlike PH-LHD, where underlying heart disease provides a clinical context for evaluation, idiopathic PAH offers no obvious underlying cause to prompt investigation. Also, the condition frequently strikes younger patients – often women between their 30s and 60s, where cardiovascular disease isn't typically suspected. This may pose an issue for women in childbearing age. Pregnancy is generally discouraged in patients with PAH, as it is associated with a high mortality rate, estimated between 30-56%.

"Problem one is that they're huffing and puffing, having shortness of breath, swelling up, but they don't seek out medical attention because they're relatively young and otherwise healthy," says Oliveros. The average age of patients with a new diagnosis of PAH in current registries is 62 years; prevalence remains female predominant.
"The other issue is that when they go to their primary care physicians, they're told, 'oh, you have asthma, or allergies, or deconditioning, or anxiety.' By the time they get to a HF specialist, they're often already in WHO functional class III or IV."
At that point, prognosis is poor and treatment is obtrusive, to put it mildly. "Depending on severity, we may directly proceed to IV infusions or subcutaneous infusions, or a combination of pills and inhalers, all of which have a lot of side effects," says Oliveros. "And that's before starting with the prior authorizations, specialized pharmacy, and all the rest of it."
The Sotatercept Breakthrough
The most significant breakthrough in PAH treatment – possibly ever – came with the FDA approval of sotatercept in March 2024. This fusion protein and first-in-class activin signaling inhibitor represents a paradigm shift from symptom management to disease modification.
Unlike traditional PAH therapies that primarily address vasoconstriction with secondary anti-remodeling effects, sotatercept addresses the fundamental problem of excessive cellular proliferation in pulmonary arteries by improving the balance between pro-proliferative and anti-proliferative signaling. Preclinical models showing cellular changes associated with thinner vessel walls, partial reversal of right ventricular remodeling and improved hemodynamics.
An Evidence Trifecta: Moderate, Early and Advanced PAH
Three pivotal phase 3 clinical trials have established the safety and efficacy of sotatercept in PAH. The first, STELLAR, provided foundational evidence that led to the drug's FDA approval.1 This multicenter, double-blind study enrolled 323 adults with WHO functional class II or III PAH who were receiving stable background therapy.
Sotatercept given subcutaneously every three weeks significantly improved exercise capacity compared to placebo (median change from baseline at week 24, 34.4 m vs. 1.0 m for placebo; difference, 40.8 m; p<0.001), while also demonstrating benefits in pulmonary vascular resistance, WHO functional class and NT-proBNP levels.
The second phase 3 trial, dubbed HYPERION, explored sotatercept's potential in newly diagnosed PAH patients at intermediate or high risk of disease progression. This global study enrolled 320 patients diagnosed within 12 months of screening.
HYPERION was stopped early after the overwhelming efficacy demonstrated in STELLAR and the release of interim results from the ZENITH trial created a loss of clinical equipoise. The trial met its primary endpoint of reducing time to clinical worsening, with full results anticipated later.
As Cardiology went to press, the full results of HYPERION were published in NEJM.2 At a median follow-up of 13.2 months, clinical worsening was seen in 10.6% of the sotatercept group, compared to 36.9% of the placebo group (hazard ratio, 0.24; p<0.001). Deterioration in exercise performance due to PAH was noted in 5.0% and 28.8%, respectively, and unplanned hospitalization for worsening PAH in 1.9% and 8.8%, respectively. Death from any cause was reported in 4.4% of the sotatercept arm and 3.8% of controls. The most common adverse events associated with the study drug were epistaxis (31.9%) and telangiectasia (26.2%).
The ZENITH trial, presented at ACC.25 and simultaneously published in NEJM, targeted high-risk patients (WHO functional class III or IV disease), and a high one-year risk of death who were receiving maximum tolerated background therapy.3 Add-on sotatercept or placebo was given to 172 patients every three weeks. ZENITH evaluated a composite primary endpoint of death, lung transplantation or PAH-related hospitalization.
"ZENITH was important because, despite the clear successes of earlier trials of sotatercept, skepticism remained about whether sotatercept, or any therapy, could meaningfully improve outcomes in patients with advanced-stage PAH, which is often regarded as highly differentiated and clinically unstable," says Bradley A. Maron, MD, FACC, director of the Pulmonary Hypertension Program at the University of Maryland, and a leading physician-scientists in PH, whose work has contributed to changing the definition of PH.
On the basis of the results of the interim analysis of the primary endpoint, ZENITH was also terminated early for overwhelming efficacy. All participants who completed the ZENITH trial were offered access to the open-label SOTERIA extension study, according to Merck.
At a median follow-up of 10.6 months, sotatercept reduced the relative risk of major morbidity and mortality events by 76% compared to placebo (17.4% vs. 54.7%; hazard ratio, 0.24; p<0.001). At the time of the data cutoff, death from any cause occurred in 8.1% of the sotatercept group and in 15.1% of the placebo arm; lung transplantation in 1.2% and 7.0%, respectively, and hospitalization for worsening PAH in 9.3% and 50.0%, respectively.
Because of the conservative p-value threshold required when the trial was terminated early (p<0.0021), the difference in the incidence of death was not significant, noted Maron in an editorial.4 "In my view, there was a clear signal towards a mortality benefit."
Treatment is associated with an increased risk of epistaxis and telangiectasias, which Maron says will need further surveillance.
"Sotatercept is clearly a major step forward and, taken together with other innovations and advances in the field, has really taken PAH out of the darkness from being a disease that is untreatable and uniformly fatal to one for which there is a multitude of different options," says Maron.
"As a result, cardiologists really need to be more aware of this disease, have a lower index of suspicion for its diagnosis, and be prepared to see patients who are on these drugs," he adds.
Walking the Walk
Oliveros has seen closeup the benefits of sotatercept. One patient went from being on an infusion pump and two oral medications and not being able to walk from the office to her car after an appointment to gardening within four months of starting sotatercept.
CTEPH: The "Curable" Form of PH
Chronic thromboembolic pulmonary hypertension (CTEPH), or Group 4 PH according to the revised clinical classification, develops when chronic blood clots obstruct pulmonary arteries, creating scar tissue that impairs blood flow. Unlike acute pulmonary emboli (PE) that can be dissolved with anticoagulation, these organized thrombi require surgical removal.
Among the five WHO groups of PH, CTEPH stands uniquely as the only potentially curable form. This distinction has gained heightened clinical significance in the post-COVID era, as the pandemic's thrombotic complications raise important questions about long-term cardiovascular consequences.
The condition affects an estimated 3% of patients post-acute PE (5% in Asians), though experts believe it remains significantly underdiagnosed.6
"When you give a patient 60 meters more [on the 6-minute walk test], that might mean they can get through their grocery shopping without having to stop and rest multiple times. This is really impactful to them!" says Oliveros. "The side effect profile with sotatercept is really good, with the worst being headaches or telangiectasias – which can get bothersome – but in the overall scheme of things, obviously isn't such a big deal."
The high cost of PAH therapies, particularly novel agents like sotatercept, raises important questions about patient access and health equity. Sotatercept currently costs between $25,000 and $30,000 a month and must be taken for life; at present there are no data on outcomes after withdrawal of the medication.
The Silent Majority: PH-LHD
While sotatercept captures the lion's share of headlines these days, cardiologists mustn't lose sight of the elephant in the room: PH-LHD, by far the most common form of the disease encountered in clinical practice.
"If you think of PH as a pie, PH-LHD is 65-80% of the pie, while PAH is only about 10%," says Onyedika J. Ilonze, MD, FACC. He is an AHFTC specialist at Indiana University, IU Health Methodist Professional Center and a member of ACC's Heart Failure and Transplant Member Section.
PH-LHD is associated with high mortality but remains frequently underdiagnosed. The heterogeneous patient population includes individuals with heart failure with reduced ejection fraction (HFrEF), heart failure with preserved ejection fraction (HFpEF) and valvular heart disease. The disease is classified further as isolated post-capillary (Ipc-PH) or combined post- and pre-capillary PH (Cpc-PH).
A COVID-19 Connection Worth Monitoring
COVID-19's well-established association with hypercoagulability and PE has raised concerns about potential increases in CTEPH incidence.7,8 The virus triggers a prothrombotic state that can persist beyond acute illness, with documented cases of PE occurring weeks to months after initial infection.
While definitive epidemiological data on post-COVID CTEPH incidence is still emerging, the temporal relationship is concerning. Given that CTEPH typically develops six months to two years after an initial embolic event, we are possibly just beginning to see the full cardiovascular aftermath of the pandemic's peak years.
"We don't know yet, but we may start seeing more of this as people get a few more years out from COVID-19. But we also think CTEPH is under-recognized, in general, and there are a lot of people possibly suffering from poor respiratory health who have this scar tissue and just don't know it," says Oliveros.
What makes CTEPH remarkable among PH subtypes is the potential for surgical cure through pulmonary thromboendarterectomy (PTE). This complex procedure, performed at specialized centers, involves removing organized clots under deep hypothermic circulatory arrest.
Recent PTE outcomes are encouraging: a 2025 meta-analysis reports 8.4% mortality across all centers, but that falls to 1-2% at expert centers.6 UC San Diego Health, the procedure's birthplace, has performed more than 5,000 PTEs with outstanding results.
"One concern I have is that some centers that are not adequately prepared to treat this may try to remove the clot thinking it's an acute fresh clot, but they don't do a full extraction. They might just remove some of it and close up the patient," notes Oliveros. "So, there's a need in this specific population for multidisciplinary trained groups that include a PH specialist, radiologist, surgeon and an interventional cardiologist who are all trained to diagnose and treat this specific disease."
For patients unsuitable for PTE, balloon pulmonary angioplasty and targeted medical therapy with riociguat provide meaningful alternatives.
The COVID-19 pandemic underscores the importance of CTEPH awareness. The challenge lies in recognition: many COVID-related embolic events may have been subclinical, and the gradual onset of CTEPH symptoms – progressive dyspnea, fatigue and exercise intolerance – can easily be attributed to "long COVID" or deconditioning.
"People can have extensive chronic clot in their lungs and not know it's there, but they're unable to walk across the room. We do PTE and extract the whole clot, and they get dramatically better," says Oliveros.
"As people are living longer, they're more likely to have left heart disease either from cardiomyopathy, HF or valvular heart disease, and this also increases the likelihood of having PH," says Ilonze, first author on a recent State-of-the-Art review on PH-LHD published in JACC: Heart Failure.5
He suggests clinicians are not thinking enough about whether their patients with left heart pathology also might have PH. Symptoms of PH-LHD (dyspnea, fatigue, exercise intolerance) are often attributed entirely to the underlying LHD, with clinicians assuming that worsening symptoms are related to progression of HF rather than development of concomitant PH-LHD.
"Having a new drug for PAH is exciting, but it probably exacerbates this issue a little bit. There's always a tendency to look for the disease for which you have a fancy new drug and not for the disease for which you have nothing special to offer the patient."
Another possible hinderance to proper diagnosis is therapeutic nihilism: Since pulmonary vasodilators are contraindicated in PH-LHD and the newly approved and wildly effective sotatercept is only for PAH, some clinicians may feel there's limited therapeutic benefit to making the specific diagnosis, leading to less aggressive evaluation.
Also, when patients are already diagnosed with HFrEF, HFpEF or valvular disease, there's less incentive to pursue invasive hemodynamic assessment. The mindset becomes "we already know they have heart disease" rather than investigating the pulmonary vascular component, says Ilonze, a move that leaves the PH-LHD undiagnosed and unmanaged. "It's important to recognize the development of PH in addition to LHD worsens the prognosis of the preexisting LHD," he adds.
There are two patient groups where it's particularly important to "tighten up the approach to PH," notes Maron. The first is those with mitral valve disease where the presence of PH might qualify them for surgery by virtue of their PH and the second in related to the use of vasodilators.
"It's also incumbent on people who are managing LHD not to routinely prescribe pulmonary vasodilators, despite how tempting that may be, because we've seen signals of harm with those drugs in patients with PH," he says.
A comprehensive task force report from the 7th World Symposium on Pulmonary Hypertension, for which Maron served as chair and first author, identified a fundamental limitation in current approaches to PH-LHD: the tendency to apply a "one-size-fits-all" classification system across vastly different cardiac pathologies.
This broad categorization fails to capture the unique pathophysiology, prevalence patterns, prognosis and treatment responses that characterize specific LHD subtypes. Maron, et al., argues that disaggregating PH-LHD into distinct clinical entities represents a critical step toward personalized medicine and improved patient outcomes.
The therapeutic implications of disaggregation extend beyond simple to encompass fundamental differences in treatment approaches and expected outcomes.
A definitive PH diagnosis requires right heart catheterization, which according to recent data is skipped about one-quarter of the time, notes Ilonze. Paradoxically, PH-LHD is occasionally overdiagnosed because some patients get labeled with PH-LHD based on echocardiographic estimates alone, without proper hemodynamic confirmation.
The emerging role of SGLT-2 inhibitors illustrates how disaggregation would be helpful. While these medications show promise in HF populations through effects on plasma volume and inflammatory pathways, their role in valvular disease or specific cardiomyopathies remains unclear and may require subtype-specific investigation.
Too Many Patients, Too Few Specialists
The sheer volume of PH-LHD cases is overwhelming, says Ilonze. "The PH specialists cannot manage all of the patients who need us at this point, so there is a heightened need for cardiologists to have a high index of suspicion for PH and be better equipped to help manage it."
He recommends a shared care model. "If a patient has PH-LHD and doesn't need specific pulmonary therapy, there can be shared care whereby the patient is seen by the local primary cardiologist but perhaps has annual visits to a specialist."
HF specialists are "critical to these efforts," if only because many PH-LHD patients have longstanding cardiomyopathies. They also play an essential role in heart transplant evaluation, optimizing guideline-directed medical therapy, and recognizing when pulmonary pressures significantly elevate procedural and surgical risk. If a patient has a severe cardiomyopathy and has developed severe PH, they are no longer a heart transplant candidate due to high perioperative mortality.
PH-LHD is prevalent in every cardiology practice whether recognized or not, says Ilonze. Every cardiologist should develop competency in recognition, have a clear referral pathway for complex cases, and understand that elevated pulmonary pressures represent a higher-risk profile that should influence clinical decision-making across the spectrum of cardiovascular care.
The Way Ahead
Sotatercept changes things for PAH, but also for the wider field. Under-recognition persists, but the advent of a breakthrough therapy puts a greater demand on clinicians to overcome educational gaps about right heart evaluation, develop comfort with PH classification and hemodynamics, and create clearer referral pathways to PH specialists.
Early diagnosis before irreversible changes occur, expanded applications of disease-modifying therapies across the PH spectrum, and continued research into approaches that target the fundamental pathophysiology rather than just symptoms represent the future of PH care.
This article was authored by Debra L Beck, MSc.
References
- Hoeper MM, Badesch DB, Ghofrani HA, et al. Phase 3 trial of sotatercept for treatment of pulmonary arterial hypertension. New Engl J Med 2023;388:1478-90.
- McLaughlin VV, Hoeper MM, Badesch DB, et al., for the HYPERION Trial Investigators. Sotatercept for pulmonary arterial hypertension within the first year after diagnosis. NEJM 2025;Published online Sept. 30: DOI: 10.1056/NEJMoa2508170.
- Humbert M, McLaughlin VV, Badesch DB, et al. Sotatercept in patients with pulmonary arterial hypertension at high risk for death. N Engl J Med 2025;392:1987-2000.
- Maron BA. Sotatercept and the clinical transformation of pulmonary arterial hypertension. N Engl J Med 2025;392:2059-61.
- Ilonze OJ, Ebong IA, Guglin M, et al. Considerations in the diagnosis and management of pulmonary hypertension associated with left heart disease. JACC: Heart Fail 2024;12:1328-42.
- Madani MM, Wiedenroth CB, Jenkins DP, Fadel E, de Perrot M. Pulmonary thromboendarterectomy: the potentially curative treatment of choice for chronic thromboembolic pulmonary hypertension. Ann Thorac Surg 2025;119:756-67.
- de Jong CMM, Visser C, Bemelmans RHH, et al. Chronic thromboembolic pulmonary hypertension and clot resolution after COVID-19-associated pulmonary embolism. Eur Respir J 2023;61:2300171.
- Reddy SA, Newman J, Leavy OC, et al. CTEPH is an uncommon complication of COVID-19: UK national surveillance and observational screening cohort studies. Eur Respir J 2024;64:2301742.
Clinical Topics: Diabetes and Cardiometabolic Disease, Heart Failure and Cardiomyopathies, Prevention, Pulmonary Hypertension and Venous Thromboembolism, Vascular Medicine, Pulmonary Hypertension, Hypertension
Keywords: Cardiology Magazine, ACC Publications, Hypertension, Pulmonary, Pulmonary Artery, Pulmonary Medicine, Vascular Remodeling