From the Member Sections | Shunt-Related Pulmonary Hypertension in Pregnancy

Pregnancies complicated by pulmonary hypertension (PH) are uncommon, however, they are associated with significant morbidity and mortality.1 Notably, 64% of pregnancies complicated by PH occur in women with underlying congenital heart disease (CHD).1 Large atrial septal defects (ASD), ventricular septal defects (VSD), atrioventricular septal defects (AVSD) or a large patent ductus arteriosus (PDA) can cause left-to-right shunting, resulting in pulmonary vascular remodeling and PH. In 1-6% of cases, severe longstanding left-to-right shunting progresses to Eisenmenger Syndrome (ES), in which rising pulmonary arterial (PA) pressures reverse shunt flow to right-to-left and cause systemic cyanosis.2,3
PH during pregnancy carries up to a 33% risk of maternal mortality, with higher rates in those with ES from CHD.4 Pregnancies in women with moderate-to-severe CHD-associated PH are linked with increased cardiac complications, including heart failure and arrhythmias, compared with women who have mild PH.5 These pregnancies have increased obstetric and fetal complications, including preeclampsia, preterm delivery, low birth weight and fetal mortality.5
Advances in preconception risk stratification, time to diagnosis and available therapies have improved outcomes; however, the morbidity and mortality burden remains high. Reproductive-aged women with established PH fall under modified World Health Organization (WHO) Class IV, with very high maternal risk of adverse events. Women with PH and a right ventricular systolic pressure RVSP ≥50 mm Hg, have at least a 10% risk of having an adverse cardiovascular event based on the CARPREG II score.6 The Zahara score specifies that women with CHD who have cyanotic heart disease or established PH with systolic PA pressure >50 mm Hg have an increased risk of cardiac complications during pregnancy.7
Understanding the Pathophysiology
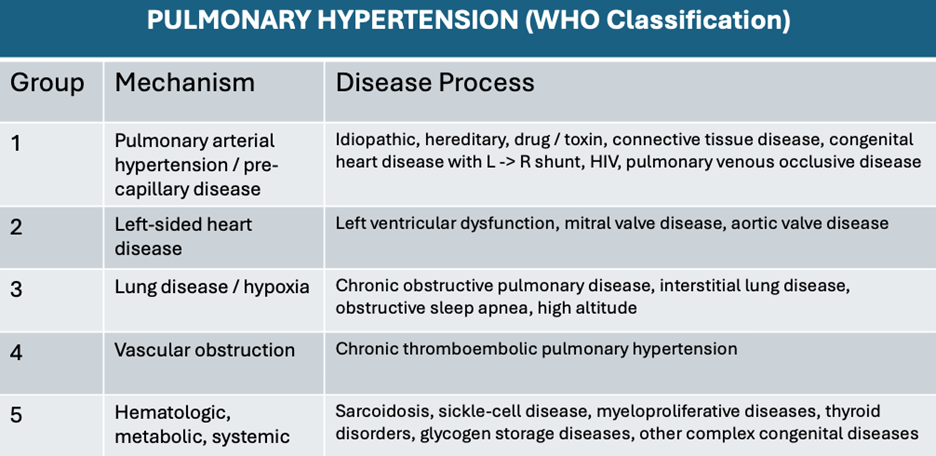
PH develops when chronic pulmonary vascular stress (e.g., increased pulmonary blood flow or pulmonary pressure, hypoxia, pulmonary vascular obstruction, primary endothelial dysfunction) leads to endothelial injury, causing PA vasoconstriction. Over time, there is smooth muscle hypertrophy, fibrosis and stiffening of pulmonary vessels, raising pulmonary vascular resistance (PVR) and PA pressures. PH is classified into five groups based on the underlying etiology (Table).
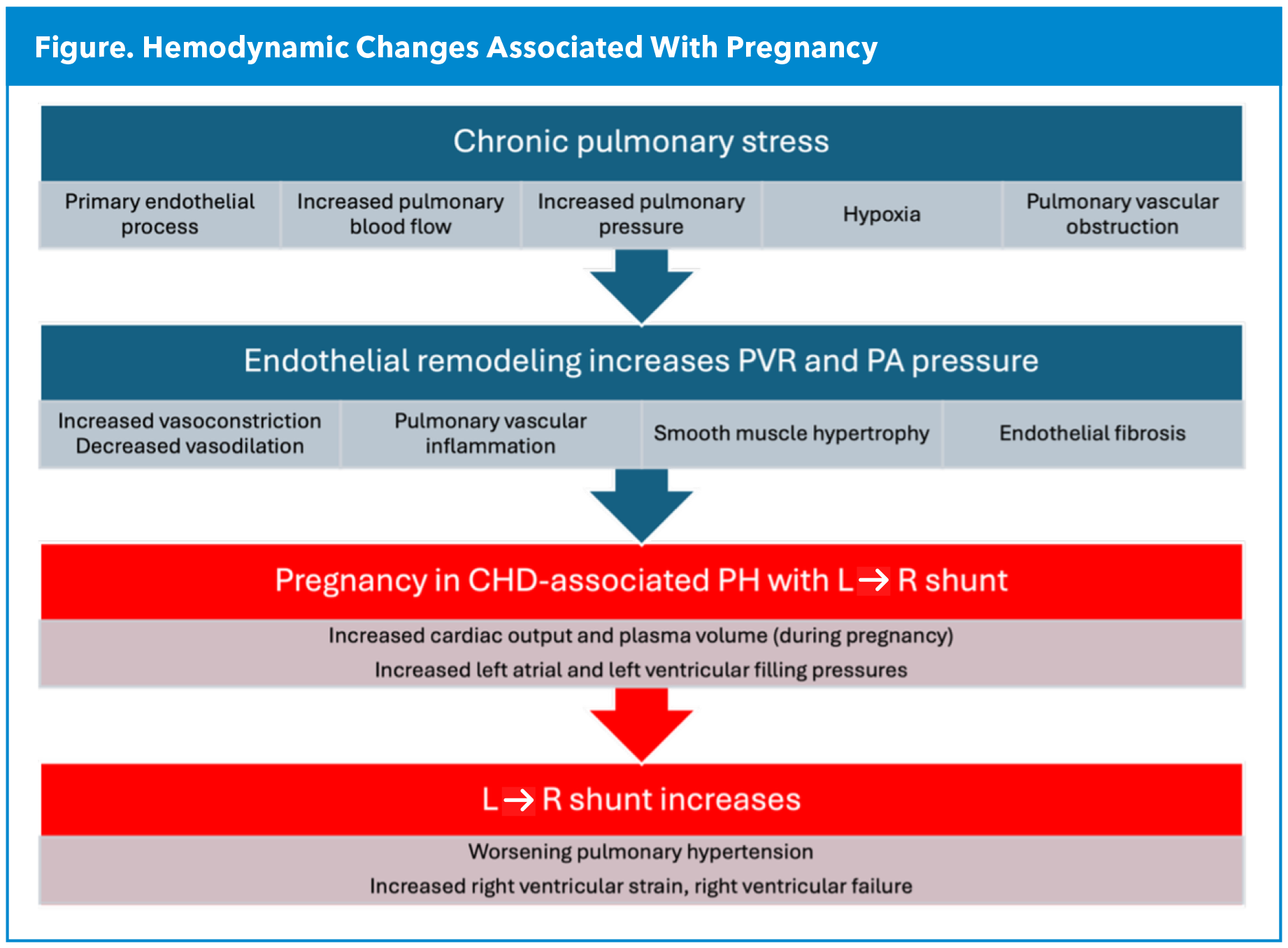
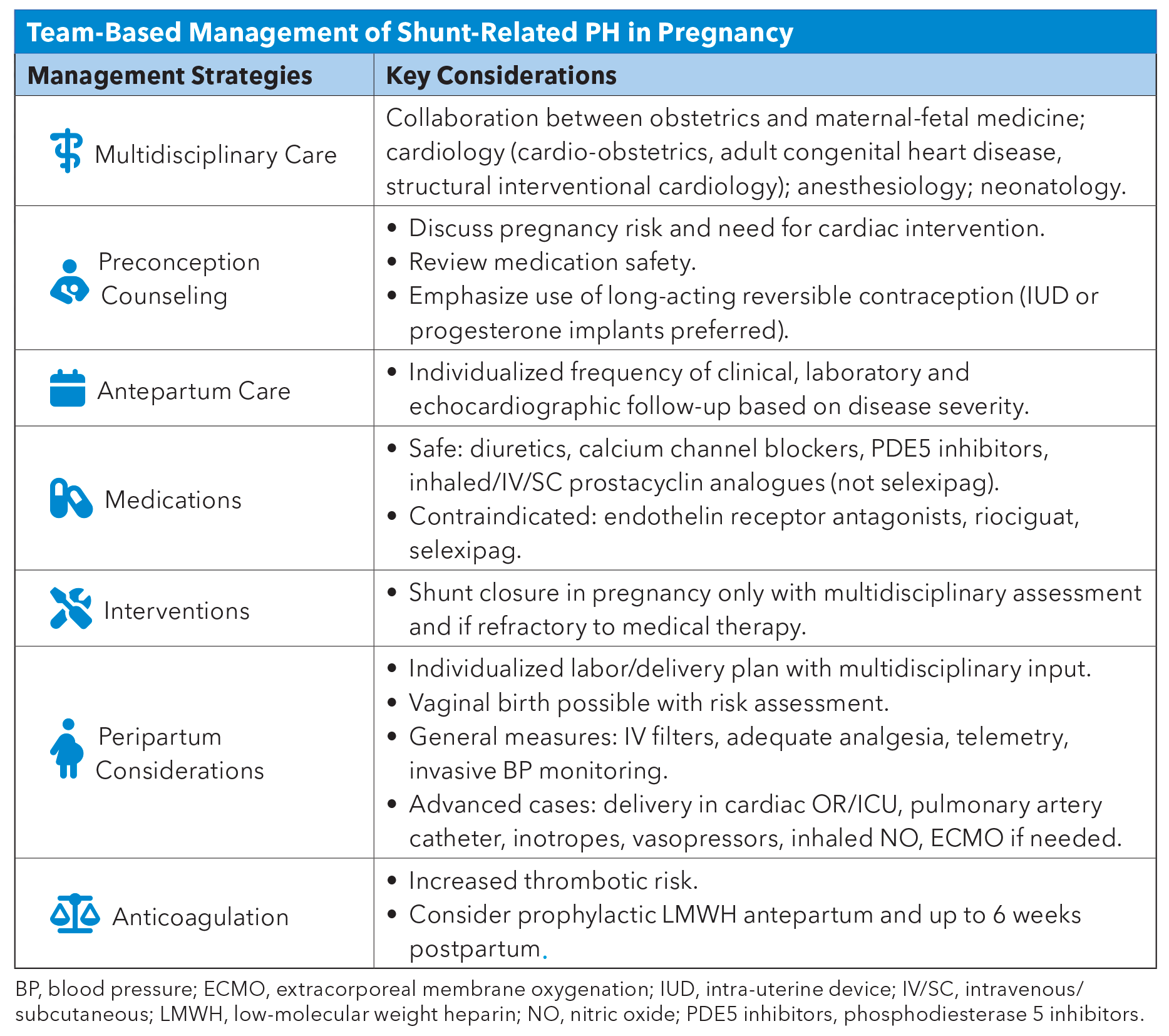
In women with CHD, pregnancy increases left-to-right shunt flow, accelerating the progression of PH (Figure). Although the relatively short period of pregnancy may not induce vascular remodeling, pregnancy-related volume shifts can acutely raise pulmonary pressures and trigger decompensation. In pregnancy, cardiac output rises by up to 50%, driven by increases in preload, stroke volume and heart rate, as well as reduction in systemic vascular resistance.8 The higher left atrial and ventricular filling pressures further augment shunt flow due to increased left-to-right gradient. In individuals with moderate-to-severe preexisting PH and elevated PVR, the additional pulmonary blood volume is poorly tolerated due to stiff, remodeled vessels. Patients with CHD-associated PH often have chronically compensated RV function, but the hemodynamic load of pregnancy can precipitate RV failure.
The Diagnostic Evaluation
The diagnosis of PH can be challenging, particularly in pregnancy, as some of the symptoms of PH overlap with those of normal gestation. Patients may report exertional dyspnea, palpitations, chest discomfort, fatigue, dizziness and peripheral edema. More advanced symptoms of abdominal distension, anorexia or early satiety and syncope are red flags for declining RV function and need urgent attention.9
On physical exam, signs of PH may include loud and palpable pulmonary component of the second heart sound, right-sided third heart sound, systolic murmur of tricuspid regurgitation that increases with inspiration (Carvallo's sign) and early diastolic murmur of pulmonary regurgitation (Graham-Steel murmur). In more advanced cases with presence of decompensated right-sided heart failure, the patient may also have jugular venous distension, ascites, peripheral edema and a pulsatile liver. For patients who present with ES, cyanosis is usually present.
The physical exam can also provide clues to the underlying cause of PH. Patients with large ASD may have a wide and fixed splitting of the second heart sound. Nonrestrictive VSDs may have a soft systolic murmur as flow is almost laminar rather than turbulent. In patent ductus arteriosus, there is a continuous machinery-like murmur with associated hyperdynamic peripheral pulses and possibly differential cyanosis of the lower extremities. Other clues on physical exam might identify an alternative etiology to PH, such as connective tissue diseases or chronic thromboembolic disease.
Laboratory investigations at diagnosis serve to identify comorbid conditions or complications of PH, and should include a complete blood count, basic chemistry and renal function, as well as liver and thyroid function. It is useful to obtain NT-proBNP levels as they correlate with prognosis in PH. Further laboratory investigations may be warranted if alternative PH etiologies are suspected.9,10
In patients with dyspnea, chest pain or syncope, it is imperative to consider pulmonary embolus and proceed with diagnostic imaging if clinically indicated, after careful discussion of risks and benefits of CT chest and/or VQ scan in pregnancy.
The initial diagnostic tool for PH is a transthoracic echocardiogram (TTE).9,10 This noninvasive, radiation-free test allows for a comprehensive assessment of cardiac function. It can help determine the presence and severity of PH. The main parameters to consider are right atrial dilatation, RV dilatation, flattening of the interventricular septum and RV dysfunction. Some other important clues include a reduced acceleration time across the pulmonic valve (<105 msec), mid-systolic notching of the RV outflow tract jet, early diastolic pulmonary regurgitation, elevated tricuspid regurgitation velocity, plethoric inferior vena cava and dilated PA. The presence of a pericardial effusion is a late finding in PH and carries a poor prognosis.
Further investigations may be warranted if alternative PH etiologies are suspected, such as high-resolution CT chest and pulmonary function tests to exclude interstitial lung disease. The risk and benefit of obtaining this test in pregnancy needs to be individualized.
Right-heart catheterization allows for obtaining valuable information in the context of PH. However, in pregnancy, invasive hemodynamics should be reserved for patients in whom medical therapy is failing, where an antepartum procedure is being considered, or in cases of diagnostic uncertainty.
A Case Study
A 25-year-old pregnant woman, with no prior antenatal care or significant past medical history, presented to the emergency department at 20 weeks of gestation for progressive dyspnea, reduced exercise tolerance and occasional palpitations over the preceding two weeks. Her vitals were blood pressure 110/70 mm Hg, heart rate 98 beats/min, respiratory rate 20 breaths/min and oxygen saturation 94% on room air. On examination, she was noted to have jugular venous distention, right ventricular (RV) heave with a fixed split S2 and a systolic ejection murmur at the left upper sternal border, clear lungs and mild lower extremity edema. Laboratory tests showed mild anemia and normal thyroid function. An electrocardiogram demonstrated right axis deviation and incomplete right bundle branch block. A transthoracic echocardiogram revealed a 2.2 cm secundum atrial septal defect (ASD) with evidence of left-to-right shunt, right atrial and RV enlargement and elevated RV systolic pressure (RVSP) concerning for pulmonary hypertension (PH).
The patient was managed conservatively with diuretics and exercise restriction, with serial clinical and echocardiographic follow-up every month. Given clinical stability, she did not require right heart catheterization. She developed symptomatic atrial flutter in the third trimester requiring cardioversion, therapeutic anticoagulation and initiation of rate control agents with low-dose metoprolol. She had no adverse perinatal outcomes. She delivered vaginally in the cardiac intensive care unit with an arterial line in situ and a titrated epidural. She will require right heart catheterization six to eight weeks after delivery to assess candidacy for ASD closure.

Learn more about ACC Member Sections and join.
References
- Afify H, Kong A, Bernal J, et al. Pulmonary hypertension in pregnancy: challenges and solutions. Integr Blood Press Control 2022;15: 33-41.
- Engelfriet PM, Duffels MG, Möller T, et al. Pulmonary arterial hypertension in adults born with a heart septal defect: the Euro Heart Survey on adult congenital heart disease. Heart 2007;93:682-87.
- Duffels MG, Engelfriet PM, Berger RM, et al. Pulmonary arterial hypertension in congenital heart disease: an epidemiologic perspective from a Dutch registry. Int J Cardiol 2007;120:198-204.
- Liu Y, Li Y, Zhang J, et al. Pregnancy outcomes of women with Eisenmenger syndrome: A single-center study. Int J Cardiol 2023; 374:35-41.
- Zhang Q, Zhu F, Shi G, et al. Maternal outcomes among pregnant women with congenital heart disease-associated pulmonary hypertension. Circulation 2023;147: 549-61.
- Silversides CK, Grewal J, Mason J, et al. Pregnancy outcomes in women with heart disease: The CARPREG II Study. J Am Coll Cardiol 2018;71:2419-30.
- Drenthen W, Boersma E, Balci A, et al. Predictors of pregnancy complications in women with congenital heart disease. Eur Heart J 2010; 31:2124-32.
- Sanghavi M, Rutherford JD. Cardiovascular physiology of pregnancy. Circulation 2014;130:1003-8.
- Humbert M, Kovacs G, Hoeper MM, et al. 2022 ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Heart J 2022;43:3618-3731.
- Stout KK, Daniels CJ, Aboulhosn JA, et al. 2018 AHA/ACC guideline for the management of adults with congenital heart disease. Circulation 2019;139:e637-e697.
Clinical Topics: Congenital Heart Disease and Pediatric Cardiology, Diabetes and Cardiometabolic Disease, Heart Failure and Cardiomyopathies, Prevention, Pulmonary Hypertension and Venous Thromboembolism, Vascular Medicine, Congenital Heart Disease, CHD and Pediatrics and Prevention, Pulmonary Hypertension, Hypertension
Keywords: Cardiology Magazine, ACC Publications, Pre-Eclampsia, Hypertension, Pulmonary, Blood Pressure, Cardio-Obstetrics, Heart Defects, Congenital, Pregnancy