Heart of Health Policy
What You Need to Know: Guidance For Clinicians on Dobutamine Shortage
The current dobutamine shortage affects multiple areas in cardiovascular medicine, including diagnostics and therapies. According to manufacturers, the crisis will be relieved in the fall of 2022 and resolved by the end of this year.
A short-acting intravenous sympathomimetic with positive inotropic and mild vasodilatory properties, the dobutamine shortage mostly impacts patients with advanced heart failure (HF) and other low output syndromes such as cardiogenic shock and early postoperative states in patients with low left ventricular ejection fraction (LVEF). Diagnostic applications such as dobutamine stress echocardiography (DSE) are also affected.
The following guidance is recommended until the dobutamine shortage is resolved:
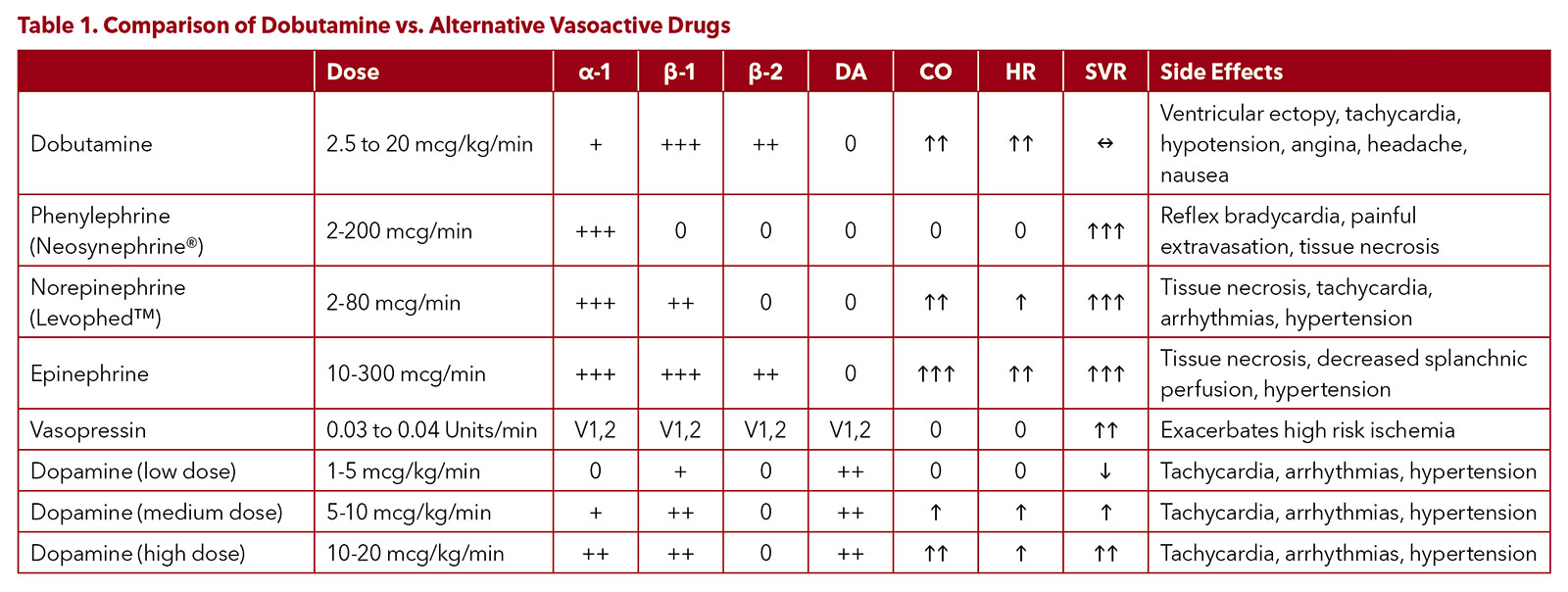
- When possible, use the alternative catecholamine or non-catecholamine inotropes and vasopressors, especially in the areas where there is no strong evidence in favor of dobutamine, such as postoperative management in patients with normal or mildly reduced cardiac output (See Table 1).
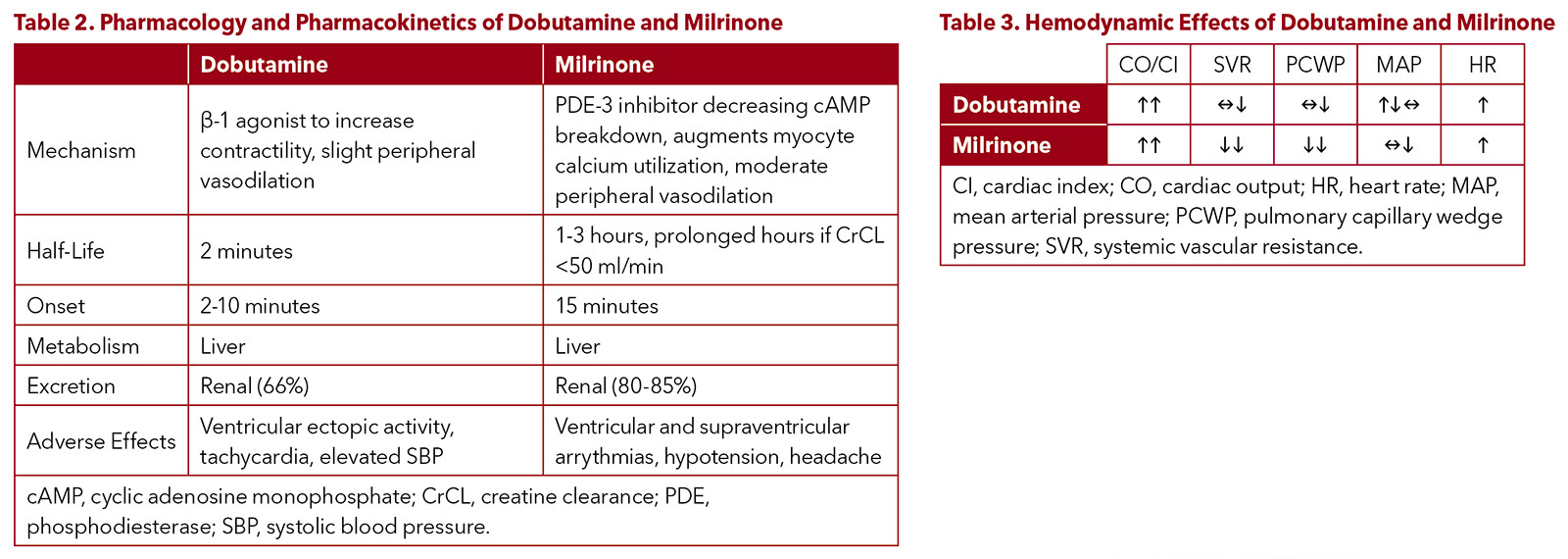
- Consider milrinone as the best alternative to dobutamine for low cardiac output conditions, including advanced HF, cardiogenic shock and postoperative states in patients with low LVEF (See Tables 2 and 3).
- Utilize other diagnostic modalities such as adenosine nuclear stress test or stress CMR for evaluation of ischemia in place of DSEs.
- Utilize other diagnostic modalities, including MRI, PET or SPECT with thallium or technetium in place of DSE to assess myocardial viability.
- No good alternatives are available for low-dose DSE, thus consider prioritizing dobutamine for this use.
Table 1 highlights the pharmacologic properties of dobutamine, a sympathomimetic amine, which acts on beta-1, beta 2 and alpha-1 adrenergic receptors. The stimulation of these receptors produces a relatively strong additive inotropic effect and a relatively weak chronotropic effect. Alpha-1 agonist activity in the vasculature causes vasoconstriction, which balances the beta-2 vasodilatory effect permitting relatively unchanged blood pressure with administration.
Tables 2 and 3 provide a pharmacological comparison of dobutamine with milrinone.
Looking Ahead
The current shortage of dobutamine creates challenges for patient care in several areas of cardiology. For some diagnostic modalities, such as DSE for risk stratification of coronary artery disease, detection of ischemia or assessment of myocardial viability, dobutamine can be replaced by alternative, mostly nonpharmacological means of testing, although with some loss in sensitivity and specificity. In postoperative care of patients who had surgery on cardiopulmonary bypass but have normal cardiac output, the shortage of dobutamine can create an opportunity to reassess the need for the routine use of vasoactive agents. Besides, there are several other agents that can be used.
It must be noted that there is no alternative to the use of dobutamine for grading the severity of low-flow aortic stenosis. Fortunately, this is a narrow area, and in most cases the test can be postponed by weeks or even months.
For the care of patients with low-output HF, the dobutamine shortage creates a very serious problem. All measures must be taken to provide an uninterrupted supply of dobutamine and milrinone. The ACC and other professional societies should use all available means including advocacy to resolve this shortage.
This document was developed by the ACC Heart Failure and Transplant Member Section, ACC Cardiovascular Team Section and University of Utah Health. Click here for the complete article, including factors contributing to the drug shortage with more details from Pfizer, and five clinical scenarios, such as evaluating ischemia, assessing myocardial viability, and low cardiac output syndrome.
Contributing authors: Maya Guglin, MD, FACC; Kristen Campbell, PharmD, FACC; Erin Fox, PharmD; Douglas Jennings, PharmD, FACC; Robert Page, PharmD; Kashif Saleem, MD; Dustin Spencer, PharmD; Barbara Wiggins, PharmD, FACC; Craig J. Beavers, PharmD, FACC.
Restrictive Covenants: What You Need to Know
Over the last decade, the shift from independent to employed/integrated practice has prompted concerns regarding restrictive covenants and noncompete clauses included in physician contracts. Not only do individual states have their own guidelines, but the potential benefits must be weighed against the potential risks to patient care, clinician well-being and the broader goal of achieving the quadruple aim.
ACC's Board of Governors (BOG) has developed a white paper designed to be a resource for ACC members and their chapters, in conjunction with legal counsel, on various aspects of the restrictive covenant issue. The white paper, which does not constitute official ACC policy, includes results from a survey of physician members conducted by the BOG and MedAxiom, along with an overview of legal perspectives, the current status of restrictive covenants in individual states, and a closer look at potential reasons to either retain restrictive covenants and/or restrict or eliminate them.
"Reasonably written restrictive covenants may facilitate practice expansion into new geographies, protect the clinical and business enterprises of the group or health system, and foster training and mentorship of new partners," the authors write. In addition, "restrictive covenants may also protect the public from the loss of specialty physicians in underserved areas and ensure that physicians are available for emergency cardiac care in specific communities."
However, the authors also note that "several arguments exist in favor of eliminating or limiting restrictive covenants." Among the concerns: potential negative impacts on contract negotiations, patient access to care, and progress towards meeting the quadruple aim and improving clinician well-being. According to the paper, the majority of survey respondents supported ACC Chapters advocating for legislation that would "limit or ban restrictive covenants."
Click here to read the complete white paper.
Click here to download a chart with state-by-state information on restrictive covenants.
Keywords: ACC Publications, Cardiology Magazine, ACC Advocacy, Health Policy
< Back to Listings