Cover Story | ACC.26: Big Easy Energy and CV Excellence
Jump to: ACC.26 Science: Moving Patient Care Forward
ACC.26: Big Easy Energy and CV Excellence
In true New Orleans style, ACC.26 delivered a dynamic, all-encompassing experience that blended cutting-edge science, immersive education and a strong sense of community across the global cardiovascular field.
Celebration, reflection and forward-looking vision was center stage over the course of the three-day event – providing thousands of cardiovascular professionals with countless opportunities to learn, share and connect.
"This meeting is intentionally designed to pull you in at every turn...so that you can return home with knowledge that you can put into practice on Tuesday morning," said ACC Scientific Session Chair Katie Berlacher, MD, FACC. "It has been a journey filled with innovation, transformation, challenge, creativity and so much joy. I could not be prouder of what we accomplished."







ACC.26 Science: Moving Patient Care Forward
ACC.26 delivered a "heard it here first" glimpse at the science poised to reshape cardiovascular care. From interventional insights and advances in structural heart and heart failure to growing evidence on Food as Medicine and community-based approaches, these late-breaking findings are already influencing what comes next.
In the first study to compare ultrasound-facilitated, catheter-directed fibrinolysis plus anticoagulation vs. anticoagulation alone in patients with acute, intermediate-risk pulmonary embolism (PE), HI-PEITHO showed that the catheter intervention led to a lower risk of the primary composite endpoint of PE-related death, cardiorespiratory decompensation or collapse, or symptomatic PE recurrence within seven days of randomization. Among 544 patients who also had two indicators of clinical severity, half were randomized to catheter treatment and half to standard systemic anticoagulation: 4% and 10.3% of each arm experienced a primary outcome at 30 days. The 61% between-arm difference significantly favored the catheter-based treatment arm and was driven by a reduction in cardiorespiratory decompensation or collapse. There were few deaths in either arm, no brain bleeds, and no significant difference in all-cause deaths or major bleeding complications. "If the right patients are selected for this procedure, it can prevent patients from deteriorating and it can do so at an acceptably low risk of bleeding complications," said Stavros V. Konstantinides, MD, PhD.
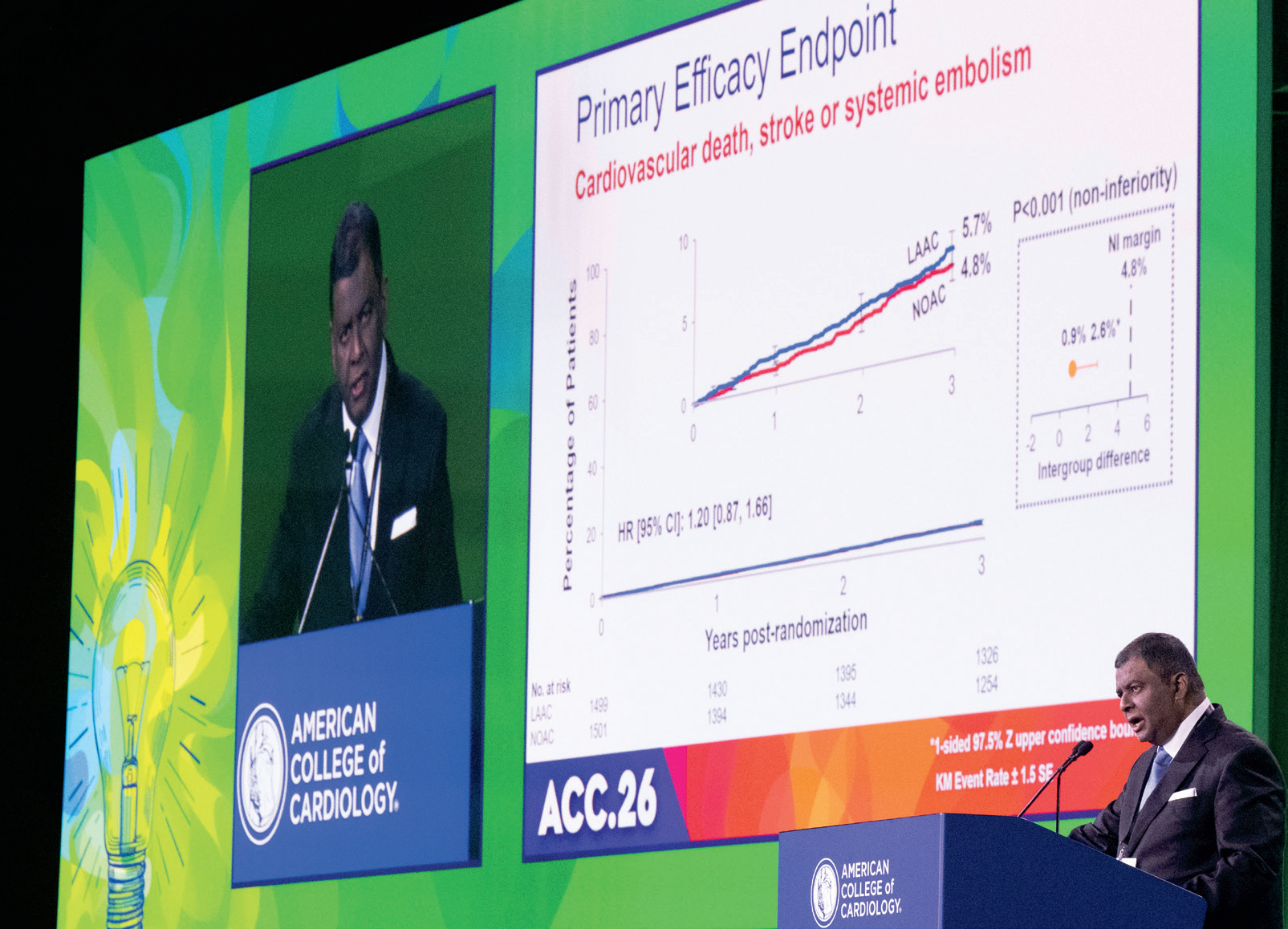
In another first, the noninferiority CHAMPION-AF trial showed that device-based left atrial appendage closure (LAAC) was comparable to non-vitamin K antagonist oral anticoagulant (NOAC) therapy in reducing the combined rate of death from cardiovascular causes, stroke or systemic embolism at three years in patients with nonvalvular atrial fibrillation (AFib) who were candidates for anticoagulation. LAAC also was superior to long-term NOAC therapy for prespecified non–procedure-related bleeding. In the multinational trial of 3,000 patients, a primary outcome occurred in 5.7% and 4.8% of the patients in the LAAC group with the WATCHMAN FLX device and NOAC group at three years. "This is an important finding because we studied people who we thought were good candidates for blood thinners," said Saibal Kar, MD, FACC, co-principal investigator. "They are not contraindicated for long-term anticoagulation and they have a low bleeding risk; in spite of that, they had increased bleeding over time."

In STEMI-DTU, compared with immediate PCI alone, the combination of mechanical left ventricular (LV) unloading using a transvalvular micro-axial flow pump (TVmAFP) plus delayed PCI did not reduce infarct size in patients with anterior STEMI without cardiogenic shock. Among 527 adults without a prior myocardial infarction (MI) in the multinational trial, 30 minutes of LV unloading before PCI vs. PCI alone resulted in no significant difference in the extent of heart-muscle damage in the two arms (30.8% and 31.9%, respectively). The 30-day rate of device-related major bleeding or blood vessel complications was 30.8% in the intervention group, exceeding the 26.5% predefined performance goal. Bleeding rates were significantly higher in the TVmAFP arm (34% vs. 6% PCI alone). Gregg W. Stone, MD, FACC, co-author of the trial, said that while the study did not meet its primary endpoint, the findings suggest several avenues for further research. Read more in JACC.
Unloading the LV before complex PCI in CHIP-BCIS3 did not reduce the risk of major adverse clinical outcomes in patients with severe LV dysfunction (LVEF ≤35%) and carried a greater risk of all-cause and cardiovascular mortality. "Our findings strongly suggest that we shouldn't be using this device routinely without more evidence of benefit," said Divaka Perera, MD, first author of the study. The open-label trial conducted in the UK found more patients who had elective unloading with a micro-axial flow pump vs. standard of care experienced the primary outcome (79.3% vs. 73.6%), a hierarchical composite of all-cause death, disabling stroke, spontaneous MI, cardiovascular hospitalization and periprocedural myocardial injury. Of 22,496 pairwise comparisons, 36.6% favored the micro-axial flow pump and 43.0% favored standard care, with a win ratio of 0.85 (p=0.30).

More Interventional Insights
Findings from ALL-RISE may signal a shift to angiography-derived fractional flow reserve (FFR) over the traditional wire-based assessment in patients with coronary artery disease (CAD) undergoing PCI, thus providing an integrated, first-line FFR and immediate functional estimate to inform revascularization decisions. The novel FFRangio method, assisted by artificial intelligence and minimally invasive, performed the same as wire-based testing, with a similar rate of the composite primary endpoint at one year (6.9% vs. 7.1%; p<0.001 for noninferiority). No differences were observed in bleeding, acute kidney injury (AKI) or procedure-related adverse events.
Another novel technique, vFFR, was also considered an important step toward a new standard of care, showing it was noninferior to pressure-wire-based FFR in patients with intermediate coronary lesions, with the composite primary outcome occurring in 7.5% of each group, respectively. In the open-label FAST III trial, the occurrence of key secondary endpoints was also similar. Using 3D quantitative angiography, vFFR identified a higher percentage of functionally significant lesions and procedures were shorter with fewer intraprocedural complications.
Angina and quality of life were improved more with angioplasty for symptomatic single-vessel coronary chronic total occlusion (CTO) in ORBITA-CTO vs. placebo in the blinded trial of 50 patients. While the results showed that angina scores improved in the placebo group, overall results found CTO PCI led to an immediate and sustained improvement in angina symptom scores, largely due to a reduction in the number of angina episodes. On average during the 168-day follow-up, patients who received CTO PCI had 31 more angina-free days than those in the placebo group. Read the paper in JACC.
Three different trials looked at the use of IVUS guidance for PCI. In DKCRUSH VIII, when using the two-stent double-kissing crush technique for PCI to treat complex coronary artery bifurcation lesions, IVUS-guided PCI was associated with a greater reduction in target vessel failure vs. angiography-guided PCI. In contrast, in IVUS-CHIP and OPTIMAL, IVUS-guided PCI was not superior in patients with complex coronary arteries or in patients with unprotected left main CAD, respectively. Access DKCRUSH VIII in JACC.
Structural Heart Interventions
Quick Takes: Food, Funding and PCSK9s
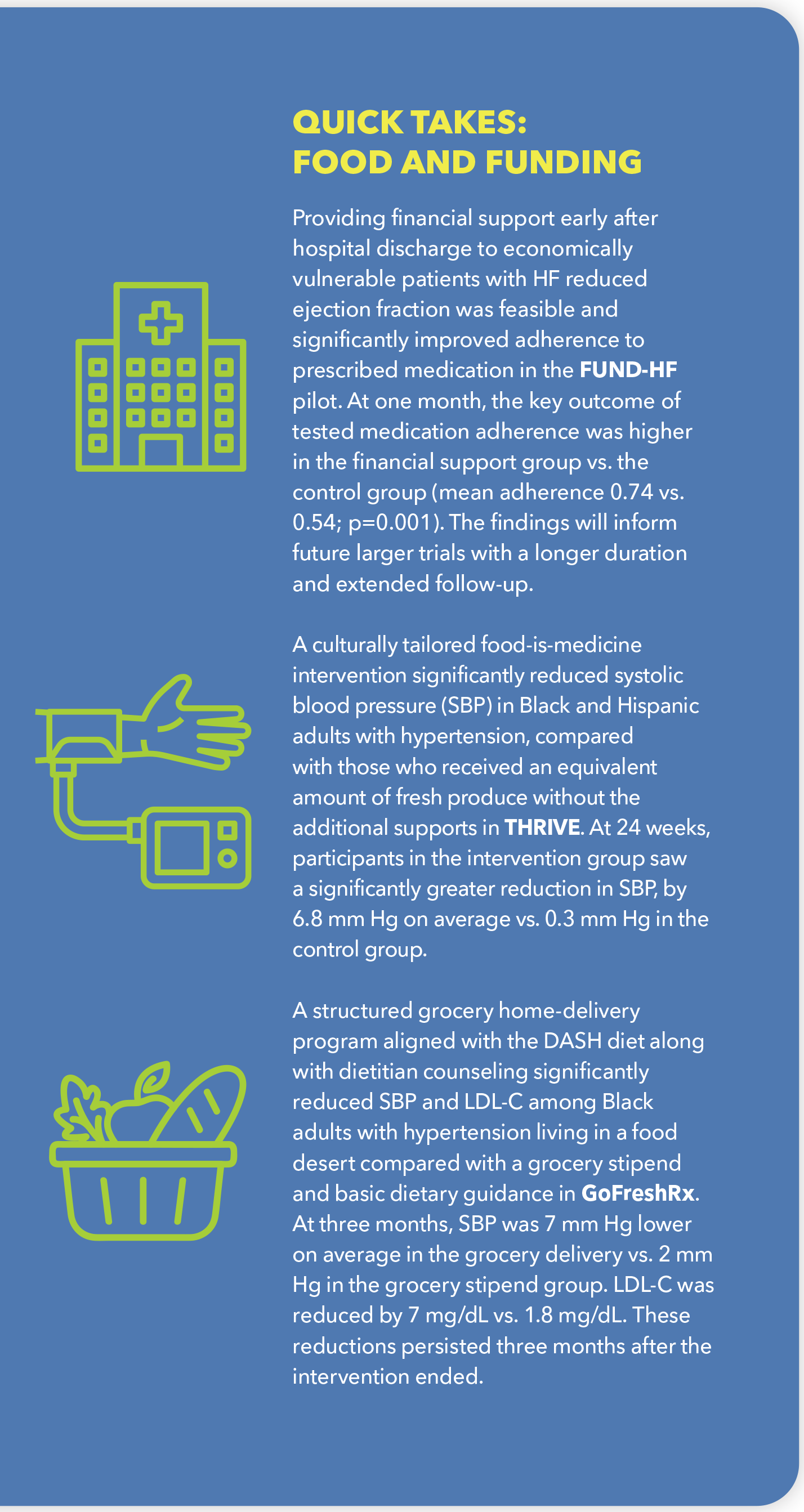
Providing financial support early after hospital discharge to economically vulnerable patients with HF reduced ejection fraction was feasible and significantly improved adherence to prescribed medication in the FUND-HF pilot. At one month, the key outcome of tested medication adherence was higher in the financial support group vs. the control group (mean adherence 0.74 vs. 0.54; p=0.001). The findings will inform future larger trials with a longer duration and extended follow-up.
A culturally tailored food-is-medicine intervention significantly reduced systolic blood pressure (SBP) in Black and Hispanic adults with hypertension, compared with those who received an equivalent amount of fresh produce without the additional supports in THRIVE. At 24 weeks, participants in the intervention group saw a significantly greater reduction in SBP, by 6.8 mm Hg on average vs. 0.3 mm Hg in the control group.
A structured grocery home-delivery program aligned with the DASH diet along with dietitian counseling significantly reduced SBP and LDL-C among Black adults with hypertension living in a food desert compared with a grocery stipend and basic dietary guidance in GoFreshRx. At three months, SBP was 7 mm Hg lower on average in the grocery delivery vs. 2 mm Hg in the grocery stipend group. LDL-C was reduced by 7 mg/dL vs. 1.8 mg/dL. These reductions persisted three months after the intervention ended.
Transcatheter tricuspid edge-to-edge repair (T-TEER) on top of standard-of-care medical therapy in TRI-FR vs. medical therapy alone reduced the risk of death, MI, stroke and hospitalization for heart failure (HF) in patients with severe symptomatic tricuspid regurgitation. At two years, 20% and 35% of the two groups, respectively, experienced a primary endpoint; 14% and 23% were hospitalized for worsening HF, representing a 40% reduction in risk.
Looking at re-do interventions, a reduction in death or disabling stroke at one year was found in SURVIV in patients with a failed mitral bioprosthetic valve who underwent transcatheter mitral valve-in-valve (mVIV) vs. a standard repeat mitral valve replacement surgery (rMVR). The study conducted in Brazil with 150 patients showed that 5.3% and 20.8% of the mVIV and rMVR groups experienced the primary endpoint. At 30 days, the rates of cardiovascular death, AKI and life-threatening or major bleeding complications were higher in the rMVR group.
Deferring PCI until after TAVI in older patients with severe aortic stenosis and substantial CAD was safe and reduced bleeding compared with PCI before TAVI in PRO-TAVI. In the deferred-PCI and PCI-first arms, there was a similar, noninferior, rate of the primary composite outcome (24% and 26%, respectively) of all-cause death, MI, stroke or moderate to severe bleeding. Notably, there was a significant difference in the rate of major bleeding at 6% in the deferred-PCI arm and 15% in the PCI-first arm, which investigators attributed to the dual antiplatelet therapy prescribed post PCI.
In PROTECT H2H, in the first head-to-head comparison of two embolic protection devices used during TAVR, the investigational Emboliner protection catheter performed comparably to the approved Sentinel cerebral protection system among 466 high-risk patients (mean age 81 years, 36% women). Results at 30 days showed that 4.9% of Emboliner patients vs. 5.0% of Sentinel patients experienced a primary endpoint event, a composite of all-cause death, stroke and acute kidney failure. Stroke within 30 days occurred in 2% and 2.1% of the two groups, "the lowest rates of stroke that have been achieved in a trial of this size," noted study author, Adam B. Greenbaum, MD, FACC. Adverse event rates were similar in both groups.
Heart Failure
In adolescents with obstructive hypertrophic cardiomyopathy (oHCM), mavacamten vs. placebo significantly improved the primary endpoint of change in Valsalva LV outflow tract gradient, with an average drop of 48.5 mm Hg vs. 0.5 mm Hg in the respective groups at 28 weeks in SCOUT-HCM. Greater improvements were also seen for secondary endpoints. Overall, 43 patients with NYHA class II or III oHCM aged 12-17 were randomized in the international trial. "Beyond symptom relief, there's a signal that this may be favorably remodeling the heart, which could improve the natural history of the disease," said first author Joseph William Rossano, MD, FACC, suggesting it could be important to start children on this therapy when they are young.
No improvement was seen with spironolactone over placebo in HF hospitalizations and cardiovascular death at 24 months in 730 patients with symptomatic HF with preserved or mildly reduced ejection fraction (HFpEF, HFmrEF) in SPIRIT-HF. The event rate of the composite primary outcome was 12.7 and 10.8 per 100-patient years in the respective groups. Notably, secondary endpoints were significantly higher in the spironolactone group, including total hospitalizations, hypotension, renal events and elevated potassium, with a trend toward increased cardiovascular hospitalizations. Noting the high rate and trend toward increased cardiovascular hospitalizations, the researchers said careful interpretation is needed because the trial is too small, yet there were some issues regarding safety and efficacy for the community to consider.
Keywords: Cardiology Magazine, ACC Publications, CM-May-2026, ACC Annual Scientific Session, ACC26, New Orleans, Awards and Prizes, Education